


pad2021_sglt2-inhibitors-glp1-agonists_handout.pdf
- 1. BC’s Provincial Academic Detailing (PAD) Service is offered free of charge to health care professionals. The service is provided by health authorities and supported by the Ministry of Health. Relevant topics are identified in consultation with various groups. All written materials are externally reviewed by clinicians and experts in critical appraisal. Type 2 Diabetes Focused Update: SGLT2 Inhibitors and GLP1 Agonists B.C. Provincial Academic Detailing (PAD) Service March 2022 updated Discuss changes to available evidence and clinical practice guidelines which inform medication choices beyond HbA1c lowering. Specifically discuss the three most commonly prescribed in British Columbia: empagliflozin, semaglutide subcutaneous, canagliflozin. Participants in this PAD session will have the opportunity to: Review clinical considerations which support treatment decisions including: doses, adverse events, dosage forms, cost and coverage.
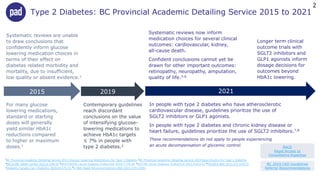
- 2. BC 2019 CKD Guidelines Referral Recommendations RACE Rapid Access to Consultative Expertise 2015 Systematic reviews are unable to draw conclusions that confidently inform glucose lowering medication choices in terms of their effect on diabetes related morbidity and mortality, due to insufficient, low quality or absent evidence.1 For many glucose lowering medications, standard or starting doses will generally yield similar HbA1c reductions compared to higher or maximum doses.1 Contemporary guidelines reach discordant conclusions on the value of intensifying glucose- lowering medications to achieve HbA1c targets ≤ 7% in people with type 2 diabetes.2 Systematic reviews now inform medication choices for several clinical outcomes: cardiovascular, kidney, all-cause death. Confident conclusions cannot yet be drawn for other important outcomes: retinopathy, neuropathy, amputation, quality of life.3-6 Longer term clinical outcome trials with SGLT2 inhibitors and GLP1 agonists inform dosage decisions for outcomes beyond HbA1c lowering. In people with type 2 diabetes who have atherosclerotic cardiovascular disease, guidelines prioritize the use of SGLT2 inhibitors or GLP1 agonists. In people with type 2 diabetes and chronic kidney disease or heart failure, guidelines prioritize the use of SGLT2 inhibitors.7,8 These recommendations do not apply to people experiencing an acute decompensation of glycemic control. 2019 2021 Type 2 Diabetes: BC Provincial Academic Detailing Service 2015 to 2021 1BC Provincial Academic Detailing Service 2015 Glucose Lowering Medications for Type 2 Diabetes 2BC Provincial Academic Detailing Service 2019 Basal Insulins for Type 2 Diabetes 3MCGUIRE JAMA Cardiol 2021;6:148-58 4KRISTENSEN Lancet Diabetes Endocrinol 2019;7:776-85 5SATTAR Lancet Diabetes Endocrinol 2021;9:653-62 6PALMER BMJ 2021;372:m4573 7Diabetes Canada Can J Diabetes 2020;44:575-91 8LI BMJ Rapid Recommendations BMJ 2021;373:n1091 2
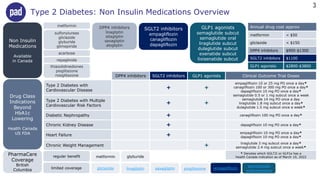
- 3. metformin sulfonylureas gliclazide glyburide glimepiride repaglinide SGLT2 inhibitors empagliflozin canagliflozin dapagliflozin GLP1 agonists semaglutide subcut semaglutide oral liraglutide subcut dulaglutide subcut exenatide subcut lixisenatide subcut Non Insulin Medications Available in Canada PharmaCare Coverage British Columbia limited coverage Annual drug cost approx metformin < $50 gliclazide < $150 DPP4 inhibitors $900-$1300 SGLT2 inhibitors $1100 GLP1 agonists $2800-$3800 gliclazide linagliptin saxagliptin pioglitazone empagliflozin semaglutide subcutaneous Drug Class Indications Beyond HbA1c Lowering Health Canada US FDA DPP4 inhibitors linagliptin sitagliptin saxagliptin alogliptin Type 2 Diabetes: Non Insulin Medications Overview acarbose 3 DPP4 inhibitors SGLT2 inhibitors GLP1 agonists Clinical Outcome Trial Doses Type 2 Diabetes with Cardiovascular Disease 🞥 🞥 empagliflozin 10 or 25 mg PO once a day* canagliflozin 100 or 300 mg PO once a day* dapagliflozin 10 mg PO once a day* semaglutide 0.5 or 1 mg subcut once a week semaglutide 14 mg PO once a day liraglutide 1.8 mg subcut once a day* dulaglutide 1.5 mg subcut once a week* Type 2 Diabetes with Multiple Cardiovascular Risk Factors 🞥 🞥 Diabetic Nephropathy 🞥 canagliflozin 100 mg PO once a day* Chronic Kidney Disease 🞥 dapagliflozin 10 mg PO once a day* Heart Failure 🞥 empagliflozin 10 mg PO once a day* dapagliflozin 10 mg PO once a day* Chronic Weight Management 🞥 liraglutide 3 mg subcut once a day* semaglutide 2.4 mg subcut once a week* * Denotes which SGLT2i or GLP1a has a Health Canada indication as of March 10, 2022 thiazolidinediones pioglitazone rosiglitazone regular benefit metformin glyburide
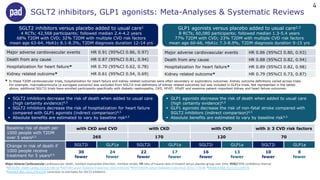
- 4. SGLT2 inhibitors versus placebo added to usual care1 4 RCTs; 42,568 participants; followed median 2.4-4.2 years 68% T2DM with CVD; 32% T2DM with multiple CVD risk factors mean age 63-64, HbA1c 8.1-8.3%, T2DM diagnosis duration 12-14 yrs Major adverse cardiovascular events HR 0.91 (95%CI 0.86, 0.97) Death from any cause HR 0.87 (95%CI 0.81, 0.94) Hospitalization for heart failure* HR 0.70 (95%CI 0.62, 0.78) Kidney related outcome* HR 0.61 (95%CI 0.54, 0.69) Major adverse cardiovascular events HR 0.86 (95%CI 0.80, 0.93) Death from any cause HR 0.88 (95%CI 0.82, 0.94) Hospitalization for heart failure* HR 0.89 (95%CI 0.82, 0.98) Kidney related outcome* HR 0.79 (95%CI 0.73, 0.87) SGLT2 inhibitors, GLP1 agonists: Meta-Analyses & Systematic Reviews Baseline risk of death per 1000 people with T2DM over 5 years4,5 with CKD and CVD with CKD with CVD with ≥ 3 CVD risk factors 265 170 120 70 Change in risk of death if 1000 people receive treatment for 5 years4,5 SGLT2i GLP1a SGLT2i GLP1a SGLT2i GLP1a SGLT2i GLP1a 30 fewer 24 fewer 22 fewer 17 fewer 16 fewer 13 fewer 10 fewer 8 fewer  SGLT2 inhibitors decrease the risk of death when added to usual care (high certainty evidence)4,5  SGLT2 inhibitors decrease the risk of hospitalization for heart failure compared with GLP1 agonists (indirect comparison)4,5  Absolute benefits are estimated to vary by baseline risk4,5  GLP1 agonists decrease the risk of death when added to usual care (high certainty evidence)4,5  GLP1 agonists decrease the risk of non-fatal stroke compared with SGLT2 inhibitors (indirect comparison)4,5  Absolute benefits are estimated to vary by baseline risk4,5 * In these T2DM cardiovascular trials, hospitalization for heart failure and kidney related outcomes were often secondary or exploratory outcomes. Kidney outcome definitions varied across trials. For example, macroalbuminuria (a surrogate outcome) was excluded from SGLT2i trial definitions of kidney related outcomes but was included in GLP1a trials. Not represented in the tables above, additional SGLT2i trials have enrolled participants specifically with diabetic nephropathy, CKD, HFrEF, HFpEF and examine patient-important kidney and heart failure outcomes. GLP1 agonists versus placebo added to usual care2,3 8 RCTs; 60,080 participants; followed median 1.3-5.4 years 77% T2DM with CVD; 23% T2DM with multiple CVD risk factors mean age 60-66, HbA1c 7.3-8.9%, T2DM diagnosis duration 9-15 yrs 4 Major Adverse Cardiovascular cardiovascular death, nonfatal myocardial infarction, nonfatal stroke; HR ratio of hazard rates in treated versus placebo group over time; 95%CI 95% confidence interval 1MCGUIRE JAMA Cardiol 2021;6:148-58 2SATTAR Lancet Diabetes Endocrinol 2021;9:653-62 3KRISTENSEN Lancet Diabetes Endocrinol 2019;7:776-85 4PALMER BMJ 2021;372:m4573 5PALMER BMJ 2022;376:o109 correction to estimates for SGLT2 inhibitors
- 5. Empagliflozin, Semaglutide subcut, Canagliflozin: Trials, Dose, Cost Type 2 Diabetes Clinical Outcome Trials HbA1c, Body Weight Ongoing Trials Empagliflozin Jardiance ~$1100 per year T2DM Cardiovascular Trial 7020 people, median follow up 3.1 years (EMPA REG 2015)1 100% CVD, mean age 63, mean HbA1c 8.1%, eGFR ≥ 30 10 or 25 mg PO once a day added to usual care When added to metformin5 ▼ HbA1c ~0.6% 25 mg vs 10 mg6 ▼ HbA1c additional 0.06-0.13% Body Weight1,7 ▼ ~2 kg Chronic Kidney Disease10 empagliflozin 10 mg Acute Myocardial Infarction11 empagliflozin 10 mg Major Adverse Cardiovascular Events: ▼ HR 0.86, 95%CI 0.74 to 0.99 ~7 fewer people per 1000/year Death from any cause: ▼ HR 0.68, 95%CI 0.57 to 0.82 ~9 fewer deaths per 1000/year Semaglutide subcutaneous Ozempic ~$2900 per year T2DM Cardiovascular Trial 3297 people, median follow up 2.1 years (SUSTAIN-6 2016)2 83% CVD or CKD, mean age 65, mean HbA1c 8.7% 0.5 or 1 mg subcut once a week added to usual care When added to metformin5 ▼ HbA1c ~1.3% 1 mg vs 0.5 mg8 ▼ HbA1c additional 0.1-0.4% Body Weight2,7 ▼ ~4 kg (0.5 mg) ▼ ~5 kg (1 mg) Diabetic Nephropathy12 semaglutide 1 mg subcut Diabetic Retinopathy13 semaglutide 1 mg subcut T2DM Cardiovascular14 semaglutide 14 mg oral Overweight & Obesity CVD15 semaglutide 2.4 mg subcut Major Adverse Cardiovascular Events: ▼ HR 0.74, 95%CI 0.58 to 0.95 ~12 fewer people per 1000/year Death from any cause: ? HR 1.05, 95%CI 0.74 to 1.50 indeterminate result, wide 95%CI Canagliflozin Invokana ~$1100 per year T2DM Cardiovascular Trial 10142 people, median follow up 2.4 years (CANVAS 2017)3 66% CVD, mean age 63, mean HbA1c 8.2%, eGFR ≥ 30 100 or 300 mg PO once a day added to usual care When added to metformin5 ▼ HbA1c ~0.6% 300 mg vs 100 mg9 ▼ HbA1c additional 0.09-0.25% Body Weight3,7 ▼ ~2 kg Major Adverse Cardiovascular Events: ▼ HR 0.86, 95%CI 0.75 to 0.97 ~5 fewer people per 1000/year Death from any cause: ▼ HR 0.87, 95%CI 0.74 to 1.01 ~2 fewer deaths per 1000/year Diabetic Nephropathy Trial 4401 people, median follow up 2.6 years (CREDENCE 2019)4 eGFR 30-89, UACR 34-566, 50% CVD, mean HbA1c 8.3% 100 mg PO once a day added to stable ACEI or ARB ESKD, Kidney Disease Death, Cardiovascular Death: ▼ HR 0.70, 95%CI 0.59 to 0.82 ~18 fewer people per 1000/year Death from any cause: ▼ HR 0.83, 95%CI 0.68 to 1.02 ~6 fewer deaths per 1000/year CVD cardiovascular disease; CKD chronic kidney disease Major Adverse Cardiovascular Events cardiovascular death, nonfatal myocardial infarction, nonfatal stroke ESKD dialysis, renal transplantation, eGFR < 15, doubling of serum creatinine HR ratio of hazard rates in treated versus placebo group over time 95%CI 95% confidence interval Per 1000/year estimate of absolute difference between treatment and placebo if 1000 people receive the medication for one year eGFR mL/min/1.73 m2; UACR urine albumin-to-creatinine ratio mg/mmol 5 1EMPA REG OUTCOME NEJM 2015;373:2117-28 2SUSTAIN 6 NEJM 2016;375:1834-44 3CANVAS Program NEJM 2017;377:644-57 4CREDENCE NEJM 2019;380:2295-306 5TSAPAS Ann Int Med 2020;173:278-86 6FDA 2014 Review Empagliflozin 7TSAPAS Diabetes Obes Metab 2021;23:2116-24 8FDA 2017 Review Semaglutide Subcutaneous 9FDA 2013 Review Canagliflozin 10EMPA KIDNEY 2022 11EMPACT MI 2023 12FLOW 2024 13FOCUS 2027 14SOUL 2024 15SELECT 2023
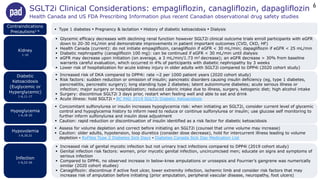
- 6. SGLT2i Clinical Considerations: empagliflozin, canagliflozin, dapagliflozin Health Canada and US FDA Prescribing Information plus recent Canadian observational drug safety studies Kidney 1-10  Type 1 diabetes ▪ Pregnancy & lactation ▪ History of diabetic ketoacidosis ▪ Dialysis Diabetic Ketoacidosis (Euglycemic or Hyperglycemic) 1-6,11-17 Infection 1-6,22-26 Hypovolemia 1-6,20,21  Glycemic efficacy decreases with declining renal function however SGLT2i clinical outcome trials enroll participants with eGFR down to 20-30 mL/min and demonstrate improvements in patient important outcomes (CVD, CKD, HF)  Health Canada (current): do not initiate empagliflozin, canagliflozin if eGFR < 30 mL/min; dapagliflozin if eGFR < 25 mL/min  Diabetic nephropathy (canagliflozin 100 mg): can be continued if eGFR < 30 mL/min until dialysis  eGFR may decrease upon initiation (on average, a 3 mL/min/1.73 m2 decrease); an eGFR decrease > 30% from baseline warrants careful evaluation, which occurred in 4% of participants with diabetic nephropathy by 3 weeks  Lower risk of hospitalization for acute kidney injury in older adults with SGLT2i compared to DPP4i (2020 cohort study)  Increased risk of DKA compared to DPP4i: rate ~2 per 1000 patient years (2020 cohort study)  Risk factors: sudden reduction or omission of insulin; pancreatic disorders causing insulin deficiency (eg, type 1 diabetes, pancreatitis, pancreatic surgery); long standing type 2 diabetes; latent autoimmune diabetes; acute serious illness or infection; major surgery or hospitalization; reduced caloric intake due to illness, surgery, ketogenic diet; high alcohol intake  Surgery: discontinue SGLT2i 3 days prior, restart when feeling well and able to eat and drink  Acute illness: hold SGLT2i ▪ BC PAD 2019 SGLT2i Diabetic Ketoacidosis Hypoglycemia 1-6,18-20  Concomitant sulfonylurea or insulin increases hypoglycemia risk: when initiating an SGLT2i, consider current level of glycemic control and hypoglycemia history to inform need to reduce or continue sulfonylurea or insulin; use glucose self monitoring to further inform sulfonylurea and insulin dose adjustment  Caution: rapid reduction or discontinuation of insulin identified as a risk factor for diabetic ketoacidosis  Increased risk of genital mycotic infection but not urinary tract infections compared to DPP4i (2019 cohort study)  Genital infection risk factors: women, prior mycotic genital infection, uncircumcised men; educate on signs and symptoms of serious infection  Compared to DPP4i, no observed increase in below-knee amputations or urosepsis and Fournier’s gangrene was numerically similar (2020 cohort studies)  Canagliflozin: discontinue if active foot ulcer, lower extremity infection, ischemic limb and consider risk factors that may increase risk of amputation before initiating (prior amputation, peripheral vascular disease, neuropathy, foot ulcers)  Assess for volume depletion and correct before initiating an SGLT2i (counsel that urine volume may increase)  Caution: older adults, hypotension, loop diuretics (consider dose decrease), hold for intercurrent illness leading to volume depletion ▪ RxFiles Type 2 Diabetes Sick Days ▪ Diabetes Canada Sick Day Medication List 6 Contraindications Precautions1-6
- 7. Subcutaneous Injection 27-29 Gastrointestinal 27-34,37,38 Hypoglycemia 27-36  Type 1 diabetes ▪ Pregnancy & lactation ▪ History of pancreatitis ▪ Concurrent DPP4 inhibitors  Personal or family history of medullary thyroid cancer, Multiple Endocrine Neoplasia syndrome type 2  Weekly: semaglutide (steady state 4-5 weeks), dulaglutide (steady state 2-4 weeks) ▪ Daily: liraglutide (steady state 3 days)  Site: abdomen, thigh, upper arm; site can be changed without dosage adjustment  Timing: any time of day, without regard to meals  Multidose disposable prefilled pen: semaglutide, liraglutide (requires pen needle change and dose selection using dose counter on pen) ▪ Single dose disposable prefilled pen: dulaglutide  Concomitant sulfonylurea or insulin increases risk: when initiating a GLP1a, consider current level of glycemic control and hypoglycemia history to inform need to reduce or continue sulfonylurea or insulin (insulin dose was decreased by 20% in semaglutide subcut trials); use glucose self monitoring to further inform sulfonylurea and insulin dose adjustment  Caution: rapid reduction or discontinuation of insulin identified as a risk factor for diabetic ketoacidosis (2019 UK Government)  Dose related: slow dose titration is intended to improve tolerability  Nausea, diarrhea >> vomiting, abdominal pain > decreased appetite > constipation, dyspepsia  Monitor for deterioration in renal function if severe adverse gastrointestinal reaction  Acute pancreatitis: discontinue GLP1a ▪ Acute gallbladder disease: gallbladder studies if cholelithiasis suspected  No observed increase in hospitalization for acute pancreatitis with incretin-based drugs (DPP4 inhibitors, GLP1 agonists) (2016 case-control study)  Increased risk in semaglutide clinical trials: monitor for progression of diabetic retinopathy in patients with retinopathy Heart Rate 27-34,38  Dose related increase in heart rate (mean increase 1-6 BPM in clinical trials); PR interval prolongation  Caution: history of tachyarrhythmias, atrioventricular block, other sympathomimetic drugs or drugs that prolong PR interval Kidney27-34  No dosage adjustment required in renal impairment; limited efficacy and safety data if eGFR < 15 mL/min or dialysis Semaglutide Oral30  Low oral bioavailability: dosed once a day on an empty stomach with maximum 120 mL of water (approx half a cup); presence of multiple tablets in the stomach decreases semaglutide absorption (wait 30 minutes before taking other oral medications) Retinopathy 27,30,31,34,38,39 GLP1a Clinical Considerations: semaglutide, liraglutide, dulaglutide Health Canada and US FDA Prescribing Information plus recent Canadian observational drug safety studies 7 Contraindications Precautions27-34
- 8. Type 2 Diabetes Focused Update: SGLT2 Inhibitors and GLP1 Agonists B.C. Provincial Academic Detailing (PAD) Service March 2022 updated Reference list is available upon request. Materials are designed to be used in conjunction with an academic detailing session provided by a PAD pharmacist. For more information, or to schedule an academic detailing session, please contact: BC Provincial Academic Detailing Service Email: PAD@gov.bc.ca Web: www.bcpad.ca This document has been compiled for the British Columbia Ministry of Health’s Pharmaceutical, Laboratory and Blood Services Division. The information contained in this document is intended for educational purposes only, and is not intended as a substitute for the advice or professional judgment of a health care professional. The information in this document is provided without any express or implied warranty regarding its content, and no party involved with the preparation of this document is responsible for any errors or omissions that may be contained herein, nor is any party involved with the preparation of this document responsible for the result obtained from the use of information in this document. Any use of this document, or the accompanying academic detailing session, will imply acknowledgement of this disclaimer and release the Province of British Columbia, its employees, agents and any party involved in the preparation of this document from any and all liability. Copyright © 2022, Province of British Columbia. All rights reserved. v. March 10, 2022