













Anatomy of Paranasal Sinuses
- 2. Introduction ’é© Air-containing spaces ’é© 4 on each side ’é© Clinically: a. Anterior : Maxillary, frontal, anterior ethmoidal (middle meatus) b. Posterior: Posterior ethmoidal (superior meatus) and sphenoidal (sphenoethmoidal recess) ’ü▒ Function: Makes skull lighter; Adds resonance
- 5. ’é© Rudimentary /absent at birth ’é© Enlarges 6-7 years ’é© Development: outpouchings from mucous membrane of lateral wall of nose.
- 6. Frontal Sinus ’é© Loc: Btw inner and outer tables of frontal bone; above and deep to supraorbital margin ’é© Asymmetric ’é© Bony septum thin & oblique ’é© 32x24x16mm ’é© Better developed in males.
- 7. ’ü▒Opens into Middle meatus ’ü▒Relations: ’ā╝ Ant : Skin over forehead ’ā╝ Posterior: Meninges + frontal lobe of brain ’ā╝ Inf: Orbit + contents ’ü▒ Drains into Frontal recess ’ü▒ Arterial supply: Supraorbital artery ’ü▒ Venous Drainage: Supraorbital and superior ophthalmic veins ’ü▒ Lymphatic: Submandibular nodes ’ü▒ Nerve: Supraorbital nerve
- 9. Maxillary Sinus ’é© Lies in body of maxilla ’é© Largest; first to develop ’é© Pyramidal; Base : med towards lat wall of nose; apex: lat in zygomatic process of maxilla ’é© Opens into middle meatus (lower part of hiatus semilunaris) ’é© Relations: Ant. Wall- Formed by facial surface of maxilla, related to soft tissues of cheek ’é© Post. Wall- infratemporal and pterygopalatine fossa
- 10. ’é© Medial wall- middle and inferior meatuses. At places uncinate process, ant and post fontanelle and inferior turbinate ’é© Floor-Alveolar and palatine processes of maxilla ’é© Roof- Floor of orbit ’é© 3.4x2.5x3.5cm ’é© Arterial: Facial, infraorbital, greater palatine arteries ’é© Venous: facial vein, pterygoid plexus ’é© Lymphatic: Submandibular nodes ’é© Nerve: Infraorbital, ant, middle, post alveolar nerves
- 11. Ethmoidal Sinus ’é© Numerous (3-18) ’é© Lie within labyrinth of ethmoid bone ’é© Relations: ’āś Above: orbital plate of frontal bone ’āś Behind: Sphenoidal conchae+ orbital process of palatine ’āś Ant: lacrimal bone ’ü▒ Divided into anterior, middle and posterior groups.
- 12. ’é© Anterior: 1-11; opens to ant part of hiatus semilunaris; Ant ethmoidal nerve + vessels; lymph ŌĆō submandibular nodes ’é© Middle: 1-7; opens to middle meatus; Post ethmoidal nerve+ vessels+ orbital branches of pterygopalatine ganglion; SM nodes ’é© Posterior: 1-7; opens to sup meatus; Post ethmoidal nerve + vessels; orbital branches of pterygopalatine ganglion; Retropharyngeal nodes.
- 14. ’é© Important cells in anterior group- Agger nasi cells, ethmoidal bulla, supraorbital cells, frontoethmoid cells, Haller cells ’é© Important cell in posterior group- Sphenoethmoid or Onodi cell
- 15. Sphenoidal Sinus ’é© Within body of sphenoid bone ’é© Separated from each by thin bony septum ’é© Asymmetric ’é© Opens to shpenoethmoidal recess ’é© Relations: ’āś Sup: Optic chiasma+ hypophysis cerebri ’āś Lat: int carotid artery+ cavernous sinus
- 16. ’ü▒ Arterial supply: Post ethmoidal + int carotid ’ü▒ Venous: Pterygoid venous plexus + cavernous sinus ’ü▒ Lymph: Retropharyngeal nodes ’ü▒ Nerve: Post ethmoidal nerve+ pterygopalatine ganglion branches.
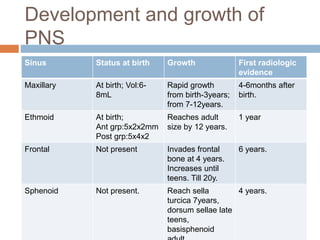
- 18. Development and growth of PNS Sinus Status at birth Growth First radiologic evidence Maxillary At birth; Vol:6- 8mL Rapid growth from birth-3years; from 7-12years. 4-6months after birth. Ethmoid At birth; Ant grp:5x2x2mm Post grp:5x4x2 Reaches adult size by 12 years. 1 year Frontal Not present Invades frontal bone at 4 years. Increases until teens. Till 20y. 6 years. Sphenoid Not present. Reach sella turcica 7years, dorsum sellae late teens, basisphenoid 4 years.
- 19. Clinical Aspects ’é© Acute Sinusitis ’é¦ acute inflammation of sinus mucosa. ’é¦ Most common: Maxillary>ethmoid>frontal>sphenoid ’é¦ Can be open/closed type- drainage of the inflammatory products into nasal cavity. ’é¦ Aetiology: ’ā╝ Exciting causes: Nasal infections, swimming and diving(bacteria, chlorine), trauma, dental infection(Max Sinus; molar/pre-molar tooth extraction)
- 20. ’éż Predisposing causes: ’āś Local: obstruction to sinus ventilation and drainage (DNS, nasal packing, hypertrophic turbinates, nasal polypi, structural abnormalities of ethmoidal air cells, neoplasm) ’āś Stasis of secretions in nasal cavity: adenoids, choanal atresia, cystic fibrosis ’āś Previous attacks of sinusitis ’é¦ General ’āś Environment:pollution, smoke, dust ’āś Poor general health: exanthematous fever, nutritional deficiency, systemic disorder
- 21. ’é© Chronic Sinusitis ’éż Sinus infection lasting for months/years Complications of sinusitis ’éż Local:Mucocele, mucous retention cyst, osteomyelitis ’éż Orbital: Preseptal inflm edema of lids, subperiosteak abscess, orbital cellulitis, orbital abscess, superior orbital fissure syndrome ’éż Intra-cranial: Meningitis, extradural abscess, subdural abscess, brain abscess, cavernous sinus thrombosis ’éż Descending infections ’éż Focal infection.
- 22. Neoplasms of PNS ’é© Benign: Osteomas, fibrous dysplasia, ossifying fibroma, ameloblastoma ’é© Malignant:Common Mostly Maxillary>ethmoid>frontal>sphenoid. 80% squamous cell type. Rest adenocarcinoma, adenoid cystic carcinoma, melanoma, sarcoma.
- 23. Thank you