1 of 62
Download to read offline
























Recommended
Disorders of the Dental Pulp.pptx
Disorders of the Dental Pulp.pptxAltilbaniHadil
╠²
This document discusses factors that affect the response of the pulp to injury, including age, inflammation, and the release of inflammatory mediators. It describes how localized inflammation can progress to pulpal necrosis if the insult is severe or prolonged enough. Pain results from the direct and indirect effects of inflammatory mediators, including lowering of sensory nerve thresholds, vasodilation, and increased tissue pressure acting on nerve receptors.PULP PERIAPICAL PATHOSIS. 111pptx.pdf
PULP PERIAPICAL PATHOSIS. 111pptx.pdfAltilbaniHadil
╠²
1. Irreversible pulpitis is an inflammatory condition of the pulp that is symptomatic or asymptomatic and caused by noxious stimuli. It can be acute or chronic.
2. Acute pulpitis is characterized by an intense inflammatory response causing teeth to be extremely sensitive to thermal changes, with hot or cold stimuli causing persisting pain.
3. Late stage irreversible pulpitis presents with throbbing pain that keeps patients awake at night, with cold providing relief and heat making the pain worse, often with referred pain and periapical changes visible on radiographs.payalseminar-150519204542-lva1-app6892.pdf
payalseminar-150519204542-lva1-app6892.pdfAltilbaniHadil
╠²
This document provides an overview of endodontic instruments used for root canal treatment. It discusses the standardization of instruments and their classification into groups based on usage. The key parts of rotary files like taper, core, flutes, cutting edges, lands and helical angles are described. It also covers various hand instruments, slow rotary instruments and their tips designs. Recent advances in nickel-titanium rotary files and their variable tapers and designs are highlighted. Instruments for different stages of root canal treatment like cleaning, shaping and obturation are also outlined.NiTi Briefly - Matt Brock(1).ppt
NiTi Briefly - Matt Brock(1).pptAltilbaniHadil
╠²
The document discusses the history and use of nickel-titanium (NiTi) alloy in endodontics. It notes that the navy initially researched NiTi in the 1950s-1960s for its non-magnetic, waterproof, and corrosion-resistant properties. NiTi was later adopted for use in orthodontics in the late 1970s and orthopedics due to its superelasticity between 10-125┬░C. The first study on using NiTi files in endodontics was published in 1988, finding they were more flexible and resistant to fractures than stainless steel. Subsequent studies in the early 1990s found NiTi hand files and rotary files required less time and caused fewer procedural errors than stainless steel.advancementsincleaningshaping-200815071852 (1).pptx
advancementsincleaningshaping-200815071852 (1).pptxAltilbaniHadil
╠²
This document discusses advancements in root canal cleaning and shaping techniques and instrumentation. It begins by outlining the disadvantages of conventional filing techniques and introduces rotary endodontic instruments as a newer technology. The document then covers the classification, history, metallurgy including nickel-titanium, and advantages of rotary instruments. It also discusses developments in nickel-titanium alloys and the components, dynamics, and importance of rotational speed for rotary instruments.endodonticmotorsandrotaryfiles-220204115618.pptx
endodonticmotorsandrotaryfiles-220204115618.pptxAltilbaniHadil
╠²
This document discusses various aspects of root canal instrumentation including the goals, hand vs rotary instrumentation, nickel-titanium files, file design features, and motor advancements. The two main goals of root canal instrumentation are to provide a biological environment conducive to healing and a canal shape that can be sealed. Rotary instrumentation has advantages over hand files like improved debris removal and following of canal anatomy. Nickel-titanium files became popular due to their flexibility and ability to return to their original shape. Key file design features that impact performance include the tip, taper, lands, flutes, helical angles, and rake angles. Modern electric motors incorporate torque control, auto-reverse functions, and apex locators to enhancedifferential_diagnosis_of_orofacial_pain.ppt
differential_diagnosis_of_orofacial_pain.pptAltilbaniHadil
╠²
This document discusses the differential diagnosis of orofacial pain from both dental and non-dental causes. It outlines various types of pain such as pulpal pain, periapical pain, referred pain, neuropathic pain, myofascial pain and others. For each type of pain, it describes characteristics such as quality, localization, reproduction of pain and response to local anesthesia. The document emphasizes taking a thorough history from the patient and considering all potential sources of pain before making a diagnosis. Diagnostic tests may include imaging, labs or use of an occlusal appliance depending on findings from history and examination.teethdiscoloration-160429235959.pdf
teethdiscoloration-160429235959.pdfAltilbaniHadil
╠²
This document discusses tooth discoloration, including its classification, etiology, and management. It covers intrinsic discoloration caused by factors like dental fluorosis, tetracycline, and certain systemic diseases. Extrinsic discoloration from substances like coffee, tea, and smoking is also addressed. Treatment options depending on the cause and severity of discoloration are presented, with bleaching and restorations discussed in detail. Vital bleaching techniques and factors affecting bleaching outcomes are also summarized.19387634-Discoloration.ppt
19387634-Discoloration.pptAltilbaniHadil
╠²
This document summarizes mechanisms of tooth staining and discoloration. It discusses how color pigments can chemically bind to dental tissues, forming new molecules that vary in size and optical effects. Natural tooth staining can be classified based on stain origin, color, and pathological versus non-pathological nature. Tooth discoloration can be associated with enamel, dentin, pulp, or combinations. The document also examines specific causes of staining like tetracycline use, fluorosis, dentinogenesis imperfecta, systemic medications, aging, and restorative materials. Treatment options mentioned include bleaching, microabrasion, veneers, and crowns.revascularization.pdf
revascularization.pdfAltilbaniHadil
╠²
1. The document discusses the management of non-vital immature permanent teeth with open apices through a revascularization procedure.
2. Revascularization involves inducing bleeding into the empty root canal to potentially trigger wound healing and regeneration of pulp tissue.
3. The procedure first disinfects the canal with irrigants and medicaments, then uses small files to induce bleeding up to 3mm into the canal, followed by placement of MTA and restoration to allow further development.Cracked Tooth Syndrome.pdf
Cracked Tooth Syndrome.pdfAltilbaniHadil
╠²
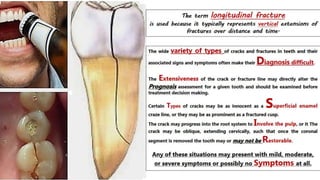
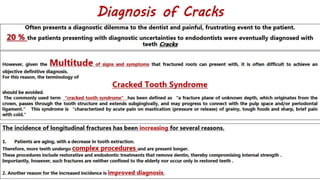
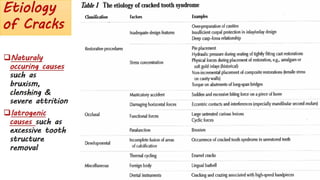
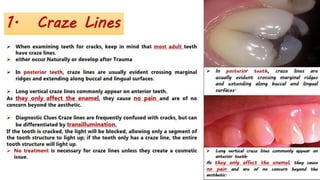
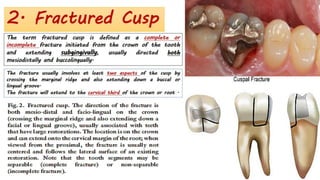
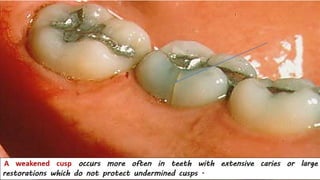
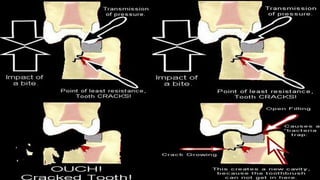
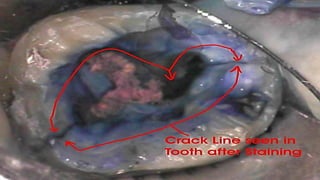
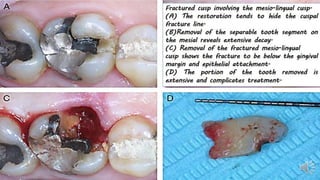
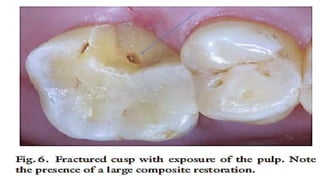
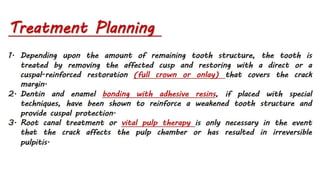
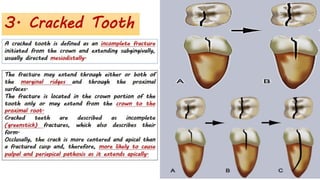
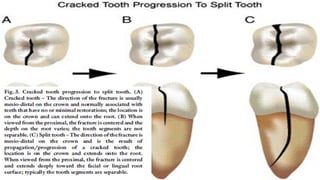
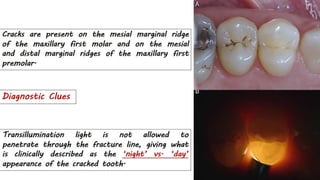
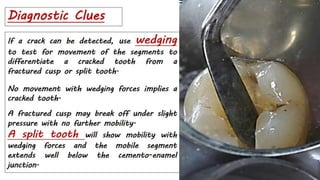
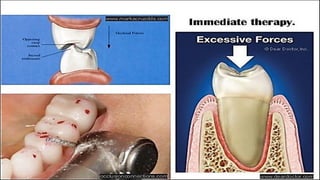
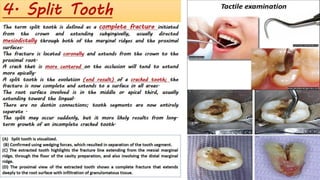
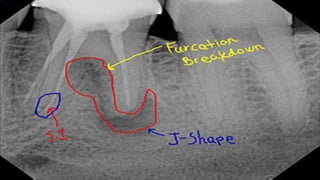
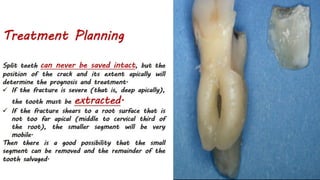
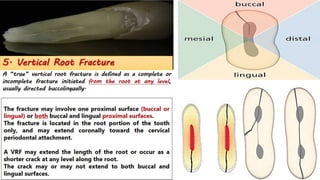
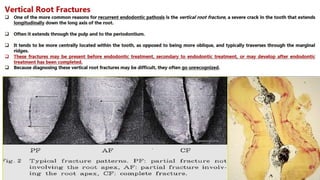
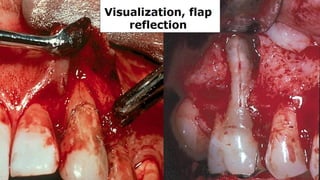
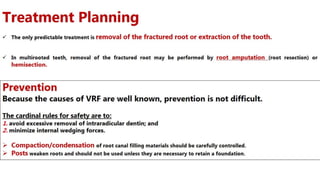
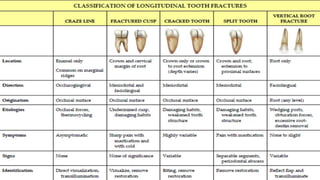
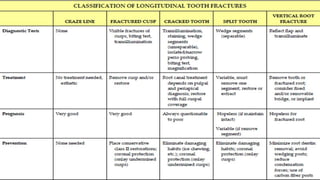
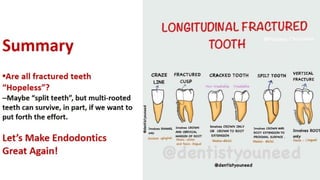
Cracked tooth syndrome is caused by a crack or break in a tooth without an associated cavity or gum disease. It causes sharp pains when biting down. Cracks often result from biting hard objects and usually occur in restored back teeth in adults. Diagnosis relies on a dental exam and history to locate the crack. Different crack types include craze lines, fractured cusps, cracked teeth, split teeth, and vertical root fractures. Treatment depends on the crack but may include splinting, root canals, or crowns to reinforce and protect the tooth. Preventing cracked teeth involves avoiding risk factors and reducing excessive forces on teeth.The traumatic dental injuries.pdf
The traumatic dental injuries.pdfAltilbaniHadil
╠²
1. Dental traumatic injuries are common, especially among children ages 2-12, and are usually caused by falls, sports accidents, or physical abuse.
2. Traumatic injuries are classified based on the affected tissues - soft tissues injuries like lacerations or fractures, tooth injuries like enamel cracks, crown fractures, root fractures, or luxation injuries.
3. The prognosis of traumatic injuries depends on factors like the patient's age, the severity of the injury, and the treatment provided. Immature permanent teeth have better prognosis than mature teeth with similar injuries.Irrigation in Endodontics.pdf
Irrigation in Endodontics.pdfAltilbaniHadil
╠²
1) Successful endodontic therapy requires thorough cleaning and disinfection of the root canal system to eliminate bacteria.
2) No single irrigant can achieve all the desired properties of dissolving tissue, disinfecting, and removing smear layer. The sequential use of sodium hypochlorite, EDTA, and chlorhexidine helps achieve through cleaning.
3) Proper irrigation technique, including using small-gauge needles, up and down motion, and replenishing irrigants, is important for disinfecting inaccessible areas of the complex root canal anatomy.pulp protection.pdf
pulp protection.pdfAltilbaniHadil
╠²
This document discusses the intimate relationship between dentin and dental pulp and how this relationship has important clinical implications. It notes that the pulp will react when dentin is injured, whether by caries, attrition, abrasion, erosion or operative procedures. It then discusses various irritants that can affect the pulp, including bacteria, iatrogenic factors like thermal changes from procedures, chemicals from materials, aging, trauma and more. It focuses on the pulpal reactions to factors like caries, local anesthetics, restorative procedures, dental materials, bleaching, periodontal procedures and orthodontic movement. It provides details on how each of these can irritate the pulp and the pulp's defensive reactions.horizontal fracture .pdf
horizontal fracture .pdfAltilbaniHadil
╠²
Horizontal root fractures represent 3% of dental traumatic injuries but have a complex healing process. Diagnosis involves clinical mobility, displacement of the coronal segment, palpation tenderness, and radiographic evidence from multiple angles. Treatment objectives are repositioning and splinting the root segments for 2-4 weeks. Prognosis depends on mobility, pulp contamination, fracture location and direction, root development stage, and time since injury. Healing can occur with calcified tissue, interproximal connective tissue, or interproximal bone and connective tissue. Complications include pulp necrosis in the coronal segment and various treatment options depend on whether segments are separated.tooth avulsion.pdf
tooth avulsion.pdfAltilbaniHadil
╠²
The document discusses traumatic dental injuries including avulsion or complete displacement of a tooth from its socket. It defines avulsion and describes the associated injuries, causes, and long term consequences. It provides details on avulsed permanent teeth including common occurrence in maxillary central incisors, higher frequency in boys than girls, and common age of 7-9 years when permanent incisors are erupting. The document discusses management of avulsed teeth including storage media to maintain viability of periodontal ligament cells, immediate replantation when possible, and follow up care and potential complications.Diagnostic Terminology.pdf
Diagnostic Terminology.pdfAltilbaniHadil
╠²
1. The document discusses diagnostic terminology and categories for pulpal and apical diagnoses as approved by endodontic organizations.
2. Several case examples are provided to demonstrate the application of diagnostic terminology. Diagnoses are made based on patient history, clinical presentation, and radiographic findings.
3. Common diagnoses include reversible and irreversible pulpitis, pulp necrosis, asymptomatic and symptomatic apical periodontitis, condensing osteitis, and previously treated teeth. Management options such as nonsurgical root canal treatment or monitoring are recommended based on the diagnoses.CLASSIFICATION (1).pdf
CLASSIFICATION (1).pdfAltilbaniHadil
╠²
The document discusses the anatomy of root canals and classifications of root canal morphologies. It introduces several past classification systems from Weine, Vertucci, and others. However, it notes that these systems are unable to categorize all the diversity seen in root canal configurations based on more recent anatomical studies using micro-CT technology. A new simplified classification system is needed that can be adopted universally to better describe the complex variations in root and root canal anatomy.ACPrep.pdf
ACPrep.pdfAltilbaniHadil
╠²
This document provides information on the morphology, root canal anatomy, and access cavities for various individual teeth. Key details include:
- The maxillary first molar typically has 3 roots (mesiobuccal, distobuccal, palatal) and 4 canals, or occasionally 3 canals. The mesiobuccal root is the most challenging to treat due to its morphology.
- The mandibular first molar usually has 3-4 canals, with two in the mesial root that are highly curved, and one or two straight canals in the distal root.
- Various teeth may have anatomical variations or anomalies, such as extra roots, fused roots, or additionalnitiendo-2-140902012325-phpapp02.pdf
nitiendo-2-140902012325-phpapp02.pdfAltilbaniHadil
╠²
This document discusses the components and design of various endodontic instruments. It describes the parts of rotary instruments like the flute, radial land, relief, helix angle, rake angle, and pitch. It then reviews the designs of different instrument types like K-files, reamers, Hedstrom files, and Gates-Glidden drills. The document also discusses modifications to traditional designs as well as newer nickel-titanium rotary systems like ProFile, LightSpeed, ProTaper, Hero, and K3. Overall, the document provides an overview of the evolution of endodontic instrument design and the key features of different instrument types.Fundamentals-of-Endodontics-lecture-20141.pdf
Fundamentals-of-Endodontics-lecture-20141.pdfAltilbaniHadil
╠²
This document provides information on a hands-on endodontics course, including key skills and factors for successful outcomes. It emphasizes the importance of thorough cleaning, shaping and obturation of the root canal system. Specific techniques discussed include using ProTaper files for canal preparation, achieving patency and gauging the apical size. Maintaining the working length within 2mm of the radiographic apex and obtaining a good coronal seal with restoration are highlighted as important factors that can influence whether endodontic treatment is successful.Treatment choices NO.ppt
Treatment choices NO.pptAltilbaniHadil
╠²
The document discusses treatment options for negative outcomes following non-surgical root canal treatment, including non-surgical retreatment, surgical retreatment, and dental implants. It reviews evidence on success rates for each option from various studies. Non-surgical retreatment can have a high success rate, particularly when there is no periapical lesion present initially. However, surgical retreatment and implants may be better options in some cases, such as when non-surgical retreatment has already failed or the anatomy makes non-surgical approaches difficult. The quality of the original root canal treatment and subsequent restoration also impact the likelihood of success. Overall, all options can have high success rates when performed by skilled operators and case selection is consideredExCath.ppt
ExCath.pptAltilbaniHadil
╠²
The document discusses the prognosis of endodontic therapy and retaining teeth. It defines prognosis as the anticipated outcome or recovery from a disease based on its usual course. The goal of endodontic treatment is to prevent and treat apical periodontitis by eliminating root canal infections. Left untreated, apical periodontitis can persist and progress from acute to chronic phases. Studies show a high prevalence of apical periodontitis, with rates varying significantly between countries. Factors like diabetes, lack of coronal coverage, and previous trauma can negatively impact prognosis. With effective treatment, the vast majority of teeth can be retained.Endo perio 2020 (1).pdf
Endo perio 2020 (1).pdfAltilbaniHadil
╠²
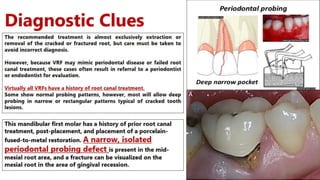
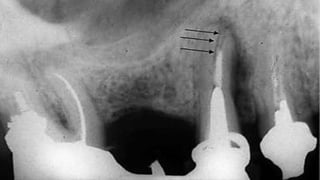
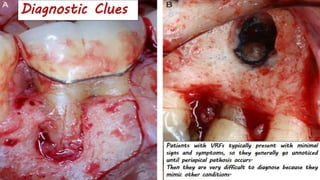
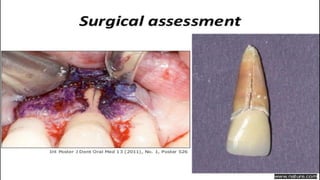
This document discusses the relationship between periodontal and endodontic diseases. It begins by establishing that the tooth, pulp, and supporting structures should be viewed as one biologic unit. There are various pathways by which communication can occur between the pulp and periodontium, including developmental pathways like lateral canals, pathological pathways caused by trauma or resorption, and iatrogenic pathways from dental procedures. Pulpal and periodontal problems are responsible for over 50% of tooth mortality. The document goes on to classify periodontal-endodontic lesions based on whether the primary source of disease is endodontic or periodontal and whether secondary involvement occurred.INTERNAL ANATOMY CLASSIFICATION.pdf
INTERNAL ANATOMY CLASSIFICATION.pdfAltilbaniHadil
╠²
This document discusses the complex anatomy of teeth, with a focus on the anatomy of the root apex. It provides background on early classification systems for tooth anatomy and describes various anatomical features of the root apex, including the apical constriction, apical foramen, types of apical constrictions, root apex shapes, canal morphologies, and root canal classifications. Understanding the detailed anatomy and variations of the root apex is important for effective endodontic treatment and procedures.HEMOLYTIC ANEMIA - thalassemia, AIHA, and NACP
HEMOLYTIC ANEMIA - thalassemia, AIHA, and NACPSSIMS & RC
╠²
Competency based classes for MBBS students.. whooping cough community health nursing.
whooping cough community health nursing.ASWIN S
╠²
Whooping cough for BSC 5th sem community health nursing..
This includes
Introduction
Definition
Incidence
Incubation period
Causes
Clinical manifestations
Diagnostic evaluation
Treatment
Prevention
Complications
Of whooping cough....THE EYELID PPT FOR 1ST YEAR BSC OPTOMETRY
THE EYELID PPT FOR 1ST YEAR BSC OPTOMETRYnihalanichz
╠²
THIS IS THE NOTES FOR EYELID ANATOMY AND SOME PHYSIOLOGY WHICH WILL HELP FOR 1ST YEAR OF BSC OPTOMETRY Update on Anesthesia for Pediatric Ophthalmic Surgery.pptx
Update on Anesthesia for Pediatric Ophthalmic Surgery.pptxDr.Umang Sharma
╠²
Based on practices on my hospital and 2021 bja articleComputer aided formulation development optimization
Computer aided formulation development optimizationSwami ramanand teerth marathwada university
╠²
Concept of optimization, optimization parameters, factorial design, optimization technology & screening design. More Related Content
More from AltilbaniHadil (17)
19387634-Discoloration.ppt
19387634-Discoloration.pptAltilbaniHadil
╠²
This document summarizes mechanisms of tooth staining and discoloration. It discusses how color pigments can chemically bind to dental tissues, forming new molecules that vary in size and optical effects. Natural tooth staining can be classified based on stain origin, color, and pathological versus non-pathological nature. Tooth discoloration can be associated with enamel, dentin, pulp, or combinations. The document also examines specific causes of staining like tetracycline use, fluorosis, dentinogenesis imperfecta, systemic medications, aging, and restorative materials. Treatment options mentioned include bleaching, microabrasion, veneers, and crowns.revascularization.pdf
revascularization.pdfAltilbaniHadil
╠²
1. The document discusses the management of non-vital immature permanent teeth with open apices through a revascularization procedure.
2. Revascularization involves inducing bleeding into the empty root canal to potentially trigger wound healing and regeneration of pulp tissue.
3. The procedure first disinfects the canal with irrigants and medicaments, then uses small files to induce bleeding up to 3mm into the canal, followed by placement of MTA and restoration to allow further development.Cracked Tooth Syndrome.pdf
Cracked Tooth Syndrome.pdfAltilbaniHadil
╠²
Cracked tooth syndrome is caused by a crack or break in a tooth without an associated cavity or gum disease. It causes sharp pains when biting down. Cracks often result from biting hard objects and usually occur in restored back teeth in adults. Diagnosis relies on a dental exam and history to locate the crack. Different crack types include craze lines, fractured cusps, cracked teeth, split teeth, and vertical root fractures. Treatment depends on the crack but may include splinting, root canals, or crowns to reinforce and protect the tooth. Preventing cracked teeth involves avoiding risk factors and reducing excessive forces on teeth.The traumatic dental injuries.pdf
The traumatic dental injuries.pdfAltilbaniHadil
╠²
1. Dental traumatic injuries are common, especially among children ages 2-12, and are usually caused by falls, sports accidents, or physical abuse.
2. Traumatic injuries are classified based on the affected tissues - soft tissues injuries like lacerations or fractures, tooth injuries like enamel cracks, crown fractures, root fractures, or luxation injuries.
3. The prognosis of traumatic injuries depends on factors like the patient's age, the severity of the injury, and the treatment provided. Immature permanent teeth have better prognosis than mature teeth with similar injuries.Irrigation in Endodontics.pdf
Irrigation in Endodontics.pdfAltilbaniHadil
╠²
1) Successful endodontic therapy requires thorough cleaning and disinfection of the root canal system to eliminate bacteria.
2) No single irrigant can achieve all the desired properties of dissolving tissue, disinfecting, and removing smear layer. The sequential use of sodium hypochlorite, EDTA, and chlorhexidine helps achieve through cleaning.
3) Proper irrigation technique, including using small-gauge needles, up and down motion, and replenishing irrigants, is important for disinfecting inaccessible areas of the complex root canal anatomy.pulp protection.pdf
pulp protection.pdfAltilbaniHadil
╠²
This document discusses the intimate relationship between dentin and dental pulp and how this relationship has important clinical implications. It notes that the pulp will react when dentin is injured, whether by caries, attrition, abrasion, erosion or operative procedures. It then discusses various irritants that can affect the pulp, including bacteria, iatrogenic factors like thermal changes from procedures, chemicals from materials, aging, trauma and more. It focuses on the pulpal reactions to factors like caries, local anesthetics, restorative procedures, dental materials, bleaching, periodontal procedures and orthodontic movement. It provides details on how each of these can irritate the pulp and the pulp's defensive reactions.horizontal fracture .pdf
horizontal fracture .pdfAltilbaniHadil
╠²
Horizontal root fractures represent 3% of dental traumatic injuries but have a complex healing process. Diagnosis involves clinical mobility, displacement of the coronal segment, palpation tenderness, and radiographic evidence from multiple angles. Treatment objectives are repositioning and splinting the root segments for 2-4 weeks. Prognosis depends on mobility, pulp contamination, fracture location and direction, root development stage, and time since injury. Healing can occur with calcified tissue, interproximal connective tissue, or interproximal bone and connective tissue. Complications include pulp necrosis in the coronal segment and various treatment options depend on whether segments are separated.tooth avulsion.pdf
tooth avulsion.pdfAltilbaniHadil
╠²
The document discusses traumatic dental injuries including avulsion or complete displacement of a tooth from its socket. It defines avulsion and describes the associated injuries, causes, and long term consequences. It provides details on avulsed permanent teeth including common occurrence in maxillary central incisors, higher frequency in boys than girls, and common age of 7-9 years when permanent incisors are erupting. The document discusses management of avulsed teeth including storage media to maintain viability of periodontal ligament cells, immediate replantation when possible, and follow up care and potential complications.Diagnostic Terminology.pdf
Diagnostic Terminology.pdfAltilbaniHadil
╠²
1. The document discusses diagnostic terminology and categories for pulpal and apical diagnoses as approved by endodontic organizations.
2. Several case examples are provided to demonstrate the application of diagnostic terminology. Diagnoses are made based on patient history, clinical presentation, and radiographic findings.
3. Common diagnoses include reversible and irreversible pulpitis, pulp necrosis, asymptomatic and symptomatic apical periodontitis, condensing osteitis, and previously treated teeth. Management options such as nonsurgical root canal treatment or monitoring are recommended based on the diagnoses.CLASSIFICATION (1).pdf
CLASSIFICATION (1).pdfAltilbaniHadil
╠²
The document discusses the anatomy of root canals and classifications of root canal morphologies. It introduces several past classification systems from Weine, Vertucci, and others. However, it notes that these systems are unable to categorize all the diversity seen in root canal configurations based on more recent anatomical studies using micro-CT technology. A new simplified classification system is needed that can be adopted universally to better describe the complex variations in root and root canal anatomy.ACPrep.pdf
ACPrep.pdfAltilbaniHadil
╠²
This document provides information on the morphology, root canal anatomy, and access cavities for various individual teeth. Key details include:
- The maxillary first molar typically has 3 roots (mesiobuccal, distobuccal, palatal) and 4 canals, or occasionally 3 canals. The mesiobuccal root is the most challenging to treat due to its morphology.
- The mandibular first molar usually has 3-4 canals, with two in the mesial root that are highly curved, and one or two straight canals in the distal root.
- Various teeth may have anatomical variations or anomalies, such as extra roots, fused roots, or additionalnitiendo-2-140902012325-phpapp02.pdf
nitiendo-2-140902012325-phpapp02.pdfAltilbaniHadil
╠²
This document discusses the components and design of various endodontic instruments. It describes the parts of rotary instruments like the flute, radial land, relief, helix angle, rake angle, and pitch. It then reviews the designs of different instrument types like K-files, reamers, Hedstrom files, and Gates-Glidden drills. The document also discusses modifications to traditional designs as well as newer nickel-titanium rotary systems like ProFile, LightSpeed, ProTaper, Hero, and K3. Overall, the document provides an overview of the evolution of endodontic instrument design and the key features of different instrument types.Fundamentals-of-Endodontics-lecture-20141.pdf
Fundamentals-of-Endodontics-lecture-20141.pdfAltilbaniHadil
╠²
This document provides information on a hands-on endodontics course, including key skills and factors for successful outcomes. It emphasizes the importance of thorough cleaning, shaping and obturation of the root canal system. Specific techniques discussed include using ProTaper files for canal preparation, achieving patency and gauging the apical size. Maintaining the working length within 2mm of the radiographic apex and obtaining a good coronal seal with restoration are highlighted as important factors that can influence whether endodontic treatment is successful.Treatment choices NO.ppt
Treatment choices NO.pptAltilbaniHadil
╠²
The document discusses treatment options for negative outcomes following non-surgical root canal treatment, including non-surgical retreatment, surgical retreatment, and dental implants. It reviews evidence on success rates for each option from various studies. Non-surgical retreatment can have a high success rate, particularly when there is no periapical lesion present initially. However, surgical retreatment and implants may be better options in some cases, such as when non-surgical retreatment has already failed or the anatomy makes non-surgical approaches difficult. The quality of the original root canal treatment and subsequent restoration also impact the likelihood of success. Overall, all options can have high success rates when performed by skilled operators and case selection is consideredExCath.ppt
ExCath.pptAltilbaniHadil
╠²
The document discusses the prognosis of endodontic therapy and retaining teeth. It defines prognosis as the anticipated outcome or recovery from a disease based on its usual course. The goal of endodontic treatment is to prevent and treat apical periodontitis by eliminating root canal infections. Left untreated, apical periodontitis can persist and progress from acute to chronic phases. Studies show a high prevalence of apical periodontitis, with rates varying significantly between countries. Factors like diabetes, lack of coronal coverage, and previous trauma can negatively impact prognosis. With effective treatment, the vast majority of teeth can be retained.Endo perio 2020 (1).pdf
Endo perio 2020 (1).pdfAltilbaniHadil
╠²
This document discusses the relationship between periodontal and endodontic diseases. It begins by establishing that the tooth, pulp, and supporting structures should be viewed as one biologic unit. There are various pathways by which communication can occur between the pulp and periodontium, including developmental pathways like lateral canals, pathological pathways caused by trauma or resorption, and iatrogenic pathways from dental procedures. Pulpal and periodontal problems are responsible for over 50% of tooth mortality. The document goes on to classify periodontal-endodontic lesions based on whether the primary source of disease is endodontic or periodontal and whether secondary involvement occurred.INTERNAL ANATOMY CLASSIFICATION.pdf
INTERNAL ANATOMY CLASSIFICATION.pdfAltilbaniHadil
╠²
This document discusses the complex anatomy of teeth, with a focus on the anatomy of the root apex. It provides background on early classification systems for tooth anatomy and describes various anatomical features of the root apex, including the apical constriction, apical foramen, types of apical constrictions, root apex shapes, canal morphologies, and root canal classifications. Understanding the detailed anatomy and variations of the root apex is important for effective endodontic treatment and procedures.Recently uploaded (20)
HEMOLYTIC ANEMIA - thalassemia, AIHA, and NACP
HEMOLYTIC ANEMIA - thalassemia, AIHA, and NACPSSIMS & RC
╠²
Competency based classes for MBBS students.. whooping cough community health nursing.
whooping cough community health nursing.ASWIN S
╠²
Whooping cough for BSC 5th sem community health nursing..
This includes
Introduction
Definition
Incidence
Incubation period
Causes
Clinical manifestations
Diagnostic evaluation
Treatment
Prevention
Complications
Of whooping cough....THE EYELID PPT FOR 1ST YEAR BSC OPTOMETRY
THE EYELID PPT FOR 1ST YEAR BSC OPTOMETRYnihalanichz
╠²
THIS IS THE NOTES FOR EYELID ANATOMY AND SOME PHYSIOLOGY WHICH WILL HELP FOR 1ST YEAR OF BSC OPTOMETRY Update on Anesthesia for Pediatric Ophthalmic Surgery.pptx
Update on Anesthesia for Pediatric Ophthalmic Surgery.pptxDr.Umang Sharma
╠²
Based on practices on my hospital and 2021 bja articleComputer aided formulation development optimization
Computer aided formulation development optimizationSwami ramanand teerth marathwada university
╠²
Concept of optimization, optimization parameters, factorial design, optimization technology & screening design. INTERPRETATION OF LABORATORY INVESTIGATIONS.pptx
INTERPRETATION OF LABORATORY INVESTIGATIONS.pptxEliLawluvi
╠²
THE DOCUMENT SUMMARIZES THE KEY COMPONENTS OF INTERPRETING FULL BLOOD CUNTComprehensive Guide on Adsorption and Partition Chromatography Techniques
Comprehensive Guide on Adsorption and Partition Chromatography TechniquesSajini
╠²
This presentation provides an in-depth overview of chromatography, focusing on adsorption and partition chromatography. It covers the principles, methodologies, types, classification, column preparation, detection methods, advantages, disadvantages, and pharmaceutical applications. A useful resource for pharmacy students and professionals in pharmaceutical chemistry.
REFRAMING OF EXPERTISE AND INFORMATION IN HEALTH
REFRAMING OF EXPERTISE AND INFORMATION IN HEALTHTina Purnat
╠²
A talk I gave at CDIC 2025 on how information and expertise in health are being reframed and how this demands change from public health.State of the Art LVAD Care: What Does the Year 2025 Bring?
State of the Art LVAD Care: What Does the Year 2025 Bring?Duke Heart
╠²
Elizabeth Volz, MD
University of North Carolina-Chapel HillAbnormal Uterine Bleeding and its Management
Abnormal Uterine Bleeding and its ManagementChandrika Kulkarni
╠²
Abnormal Uterine Bleeding and its ManagementUnlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions
Unlocking the Potential of Long-Acting PrEP to Halt HIV TransmissionsPVI, PeerView Institute for Medical Education
╠²
Chair, Allison Agwu, MD, ScM, FAAP, FIDSA, discusses HIV in this CME/MOC/NCPD/CPE/AAPA/IPCE activity titled ŌĆ£Unlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions.ŌĆØ For the full presentation, downloadable Practice Aids, and complete CME/MOC/NCPD/CPE/AAPA/IPCE information, and to apply for credit, please visit us at https://bit.ly/40Mr2AC. CME/MOC/NCPD/CPE/AAPA/IPCE credit will be available until June 12, 2026.Day care surgery anaesthesia and management of complications in postoperative...
Day care surgery anaesthesia and management of complications in postoperative...deepika582423
╠²
Day care 5-Lift Analysis in ergonomics focuses on evaluating the safety and efficienc...
5-Lift Analysis in ergonomics focuses on evaluating the safety and efficienc...Bolan University of Medical and Health Sciences ,Quetta
╠²
Lift Analysis in ergonomics focuses on evaluating the safety and efficiency of manual lifting tasks in the workplace. It involves assessing the physical demands placed on the human body during lifting activities to prevent musculoskeletal disorders (MSDs), particularly lower back injuriesHEALTH CARE PLANNING AND ORGANIZATION OF HEALTH CARE
HEALTH CARE PLANNING AND ORGANIZATION OF HEALTH CAREnawaabaquib
╠²
This PowerPoint presentation covers Unit II: Health Care Planning and Organization of Health Care at Various Levels in a simple and easy-to-understand format. It explains importance of health planning in India. The PPT also includes the structure of the health care system at central, state, and local levels. It is useful for GNM ,BSc And Msc Nursing students. This presentation is also helpful for exam preparation .Updates_in Head__Neck TNM staging- 9th edition.pptx
Updates_in Head__Neck TNM staging- 9th edition.pptxDr. Maroti Wadewale
╠²
The Union for International Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC) collaborate closely to produce the globally recognized TNM Classification of Malignant Tumours. Therefore, when discussing the "9th edition of UICC head and neck staging," it's largely in alignment with the updates introduced by the AJCC's Version 9. The UICC's TNM Core Committee finalized the 9th edition of the TNM Classification, with publication anticipated in August 2025.
The key updates for head and neck cancers in the 9th edition (or Version 9) reflect an ongoing effort to improve prognostic accuracy and align staging with contemporary clinical understanding and treatment outcomes. Here are the significant changes, particularly those relevant to head and neck:
* Emphasis on Personalized Care and Prognostic Refinements: The 9th edition reflects a greater focus on personalized care, incorporating refinements that aim to better predict patient outcomes.
* Revised Criteria for Specific Head and Neck Cancers:
* Nasopharyngeal Carcinoma (NPC): This site has seen substantial revisions, as highlighted in the previous response on AJCC updates. Key changes include:
* More precise definition of T3 disease (unequivocal evidence of bone involvement).
* Introduction of advanced radiologic extranodal extension (ENE) as an N3 criterion. This acknowledges the prognostic impact of ENE seen on imaging.
* Subclassification of M1 disease into M1a (3 or fewer metastatic lesions) and M1b (more than 3 lesions) to better stratify prognosis in metastatic settings.
* Redefined Stage Groups for NPC, with T1-2N0-1 now often falling into Stage I, and Stage IV being exclusively for metastatic disease, further subdivided by the M1a/M1b categories.
* Salivary Gland Cancers: Revised criteria based on updated imaging and anatomical features are being incorporated.
* HPV-Related Oropharyngeal Cancers: New staging is introduced for HPV-associated oropharyngeal cancers to better reflect their distinct biological behavior and prognosis, which is generally more favorable than HPV-negative oropharyngeal cancers. This often involves specific considerations for nodal burden.
* Integration of Imaging and Anatomical Features: The updates are grounded in recent evidence, incorporating insights from advanced imaging techniques and a deeper understanding of anatomical spread.
* International Collaboration: These updates are the result of collaborative efforts between the AJCC and UICC, involving input from cancer registries, clinical outcomes data, and disease-specific experts worldwide. The goal is to provide a unified and globally applicable staging system.
* Dynamic Update Process: Similar to the AJCC's shift from "Editions" to "Versions" for specific sites, the UICC is also exploring more flexible ways to share future TNM updates.
In essence, the 9th edition of the UICC staging system for head and neck cancers, particularly in areas like NPC and HPVCell Injuri. pathophpysiology sem- II B Pharmacypptx
Cell Injuri. pathophpysiology sem- II B PharmacypptxUmeshMali25
╠²
This presentation provides a comprehensive overview of cell injury, a fundamental concept in pathology. It covers the causes, types (reversible and irreversible), mechanisms of injury (including hypoxia, free radicals, and chemical agents), and the morphological and biochemical changes that occur during cell injury. The slides are ideal for medical, pharmacy, and life sciences students preparing for pathology coursework or exams.
ELECTROMYOGRAPHY.pptX by GOKULAKRISHNAN.
ELECTROMYOGRAPHY.pptX by GOKULAKRISHNAN.GOKULAKRISHNAN JANARTHANAN
╠²
Electromyography is basically the study of motor unit activity.
In electromyography, the study of the electrical activity of contracting muscle provides information concerning the structure and function of the motor units.
Unlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions
Unlocking the Potential of Long-Acting PrEP to Halt HIV TransmissionsPVI, PeerView Institute for Medical Education
╠²
5-Lift Analysis in ergonomics focuses on evaluating the safety and efficienc...
5-Lift Analysis in ergonomics focuses on evaluating the safety and efficienc...Bolan University of Medical and Health Sciences ,Quetta
╠²