















Headache
- 1. Evaluation of Headache in Adults Bita Fakhri, MD, MPH Boston Medical Center Shapiro Primary Care Clinic 2/27/2013
- 2. Evaluation of Headache in Adults ď‚— History ď‚— Danger signs on history ď‚— Physical exam ď‚— Danger signs on physical exam ď‚— Three main classes of primary headaches ď‚— Indications for imaging studies
- 3. History ď‚— Age at onset ď‚— Presence or absence of aura and prodrome ď‚— Frequency, intensity, and duration of attack ď‚— Number of headache days per months ď‚— Time and mode of onset ď‚— Quality, site and radiation of pain ď‚— Associated symptoms and abnormalities ď‚— Family history of migraine ď‚— Precipitating and relieving factors ď‚— Effect of activity on pain
- 4. History ď‚— Relationship with food and alcohol ď‚— Response to any previous treatment ď‚— Any recent change in vision ď‚— Association with recent trauma ď‚— Any recent changes in sleep, exercise, weight, or diet ď‚— State of general health ď‚— Change in work or life style (disability) ď‚— Change in method of birth control ď‚— Possible association with environmental factors ď‚— Effects of menstrual cycle and exogenous hormones
- 5. Danger Signs on history  Sudden onset of headache, or severe persistent headache that reaches maximal intensity within a few seconds or minutes (? SAH)  The absence of similar headaches in the past – the “first” or “worst” headache of my life (ICH, CNS infection)  A worsening pattern of headache (mass lesion, subdural hematoma, medication overuse headache)  Focal neurologic symptoms other than typical visual or sensory aura (mass lesion, AVM, collagen vascular disease)
- 6. Danger Signs on history ď‚— Fever (infection, SAH) ď‚— Any change in mental status, personality, or fluctuation in the level of consciousness ď‚— The rapid onset of headache with strenuous exercise (? Carotid artery dissection or ICH) ď‚— Head pain that spreads into the lower neck and between the shoulders may indicate meningeal irritation (infection, SAH) ď‚— New headache in patients <5 or >50
- 7. Danger Signs on history ď‚— New headache type in a patient with cancer suggests metastasis. ď‚— New headache type in a patient with Lyme disease suggests meningoencephalitis. ď‚— New headache type in a patient with HIV suggests an opportunistic infection or tumor. ď‚— Headache during pregnancy or postpartum suggests possible cortical vein or venous sinus thrombosis, carotid dissection
- 8. Physical Exam ď‚— Obtain BP and pulse ď‚— Listen for bruits at neck, eyes, and head for clinical signs of AVM ď‚— Palpate the head, neck, and shoulder regions ď‚— Check temporal and neck arteries ď‚— Examine the spine and neck muscles ď‚— Functional neurologic examination
- 9. Danger Signs on Examination ď‚— Neck stiffness and especially meningismus (resistance to neck flexion) suggests meningitis ď‚— Papilledema (intracranial mass lesion, pseudotumorcerebri, encephalitis, or meningitis) ď‚— Focal neurologic signs (intracranial mass, AVM, collagen vascular disease)
- 10. Characteristics of Common Headache Syndromes SYMPTOM MIGRAINE TENSION CLUSTER HEADACHE HEADACH HEADACHE E LOCATION Unilateral in 60- Bilateral ALWAYS 70% -- bilateral or unilateral glabal in 30% CHARACTERISTICS Gradual in onset, Pressure or Pain begins crescendo pattern; tightness that quickly, reaches a pulsating; moderate waxes and crescendo within or severe intensity; wanes minutes; pain is aggravated by deep, continuous, routine physical excruciating, and activity explosive in quality
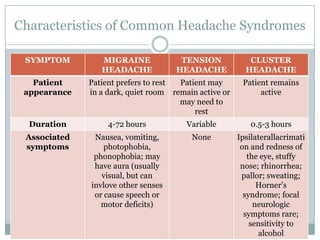
- 11. Characteristics of Common Headache Syndromes SYMPTOM MIGRAINE TENSION CLUSTER HEADACHE HEADACHE HEADACHE Patient Patient prefers to rest Patient may Patient remains appearance in a dark, quiet room remain active or active may need to rest Duration 4-72 hours Variable 0.5-3 hours Associated Nausea, vomiting, None Ipsilaterallacrimati symptoms photophobia, on and redness of phonophobia; may the eye, stuffy have aura (usually nose; rhinorrhea; visual, but can pallor; sweating; invlove other senses Horner’s or cause speech or syndrome; focal motor deficits) neurologic symptoms rare; sensitivity to alcohol
- 12. Treatment of Migraine Headaches • Abortive therapy: ASA, tylenol, caffeine, high dose NSAIDs, triptans • Prophylaxis: TCA, BB, CCB, Valproic acid, topiramate
- 13. Criteria for Transformed Migraine and Medication-Overuse Headache. Dodick DW. N Engl J Med 2006;354:158-165.
- 14. Preventive Medications Used in Cases of Transformed Migraine or Medication-Overuse Headache. Dodick DW. N Engl J Med 2006;354:158-165.
- 16. Treatment of Cluster Headaches ď‚— Acute treatment: O2, triptans ď‚— Chronic prophylaxis: CCB
- 17. Indications for Imaging Studies ď‚— Recent significant change in pattern, ferequency, or severity of headache ď‚— Progressive worsening of headache despite appropriate therapy ď‚— Focal neurologic signs and symptoms ď‚— Onset of headache with exertion, cough, or sexual activity ď‚— Orbital bruit ď‚— Onset of headache after age 40
- 18. CT vs. MRI ď‚— There is no evidence that MRI > CT ď‚— CT-brain and brainstem with and without contrast is sufficient in most patients. ď‚— MRI along with MRA are indicated when posterior fossa or vascular lesions are suspected.
- 19. The Pain of Cluster Headache ď‚— http://www.youtube.com/watch?v=glBmSQRxaIg