
1 of 36
Downloaded 64 times




Ad
Recommended
Supraventricular tachyarrythmias
Supraventricular tachyarrythmiasRawalpindi Medical College
Ěý
This document describes different types of supraventricular tachycardias (SVTs), which are rapid heart rhythms originating above the ventricles. It defines SVTs and paroxysmal supraventricular tachycardia (PSVT), and lists common symptoms. The types of SVTs are categorized based on their origin in the sinoatrial node, atria, or atrioventricular node/junction. Each type has a distinct electrocardiogram appearance and cause, such as reentry circuits, ectopic foci, or increased node automaticity. Common examples include AV nodal reentrant tachycardia, atrial fibrillation, atrial flutter, and Wolff-Parkinson-Approach to svt
Approach to svt Amir Mahmoud
Ěý
This document provides information on various types of supraventricular tachyarrhythmias including AV nodal reentrant tachycardia (AVNRT), orthodromic reciprocating tachycardia (ORT), atrial tachycardia, junctional tachycardias, Wolff-Parkinson-White (WPW) syndrome, and atrial fibrillation. It discusses the mechanisms, ECG patterns, symptoms, diagnostic approaches, and management options for these arrhythmias in 1-3 sentences per type of arrhythmia.Ecg in acs
Ecg in acsLPS Institute of Cardiology Kanpur UP India
Ěý
The document discusses electrocardiograms (ECGs) in the context of acute coronary syndrome. It begins by describing the normal conduction system and the 12 standard ECG leads. It then explains how ECGs are recorded and the positioning of limb and precordial leads. The document discusses ST segments, T waves, and how to evaluate for ST elevations. It defines acute coronary syndrome and describes the classifications of ST-elevation MI, non-ST-elevation MI, and unstable angina based on ECG and cardiac enzyme findings. Specific ECG patterns for lateral, inferior, septal, and posterior wall MIs are also shown.Ecg quiz @ SEMICON 1018
Ecg quiz @ SEMICON 1018Dr.Venugopalan Poovathum Parambil
Ěý
The document contains a detailed analysis of various case scenarios related to electrocardiograms (ECGs) and their interpretations in emergency medicine. It discusses multiple patient cases with specific symptoms and presents ECG findings along with potential diagnoses, management strategies, and critical considerations. The document serves as a comprehensive guide for emergency physicians in recognizing and responding to different cardiac conditions based on ECG readings.Tachyarrhythmias
TachyarrhythmiasSCGH ED CME
Ěý
This document provides guidance on the assessment and treatment of arrhythmias presenting in the emergency department. It outlines an approach of first determining hemodynamic stability, then distinguishing between narrow and wide complex tachycardias, and finally determining the specific arrhythmia and appropriate treatment. For unstable patients with any arrhythmia, synchronized direct current cardioversion is recommended. Further treatment is tailored based on whether the arrhythmia has narrow or wide QRS complexes and is regular or irregular.Tachyarrhythmia
TachyarrhythmiaSMSRAZA
Ěý
This document provides an overview of evaluating and treating different types of tachycardia, including:
1) It discusses evaluating the patient's hemodynamic stability, history, and ECG to determine the characteristics and cause of the tachycardia.
2) It describes differentiating between narrow and wide complex tachycardias, and the differential diagnoses for each, including sinus tachycardia, atrial fibrillation, AV nodal reentrant tachycardia, and ventricular tachycardia.
3) It provides guidance on therapies for different tachycardias, such as electrical or chemical cardioversion, rate control, and ablation. The importance of correctly diagnosing wide complex tachycardBradycardia Assessment and Management
Bradycardia Assessment and ManagementSCGH ED CME
Ěý
This document discusses the classification, causes, symptoms, and treatment of bradycardia. It defines different types of bradycardia based on rhythm and heart block. Common causes include medications, cardiac disease, metabolic abnormalities, and neurological or infectious etiologies. Symptoms range from dizziness to hypotension and shock. Treatment follows ACLS algorithms and may include atropine, transcutaneous pacing, or addressing underlying causes. Case examples demonstrate ECG findings and management of hyperkalemia-induced complete heart block, athlete's heart, and inferior STEMI with complete heart block.Constrictive pericarditis
Constrictive pericarditishodmedicine
Ěý
Constrictive pericarditis is caused by scarring and thickening of the pericardium, restricting cardiac filling. It is diagnosed using echocardiography which shows septal bounce, exaggerated mitral inflow, and hepatic vein reversal. While similar to restrictive cardiomyopathy, constrictive pericarditis shows increased ventricular interaction and respiratory effects on cardiac physiology. Surgical pericardiectomy is usually required for treatment but is high risk, with post-op complications common. Long-term survival depends on the underlying cause of constriction.tachyarrythmias d
tachyarrythmias dRavi Kanth
Ěý
This document provides an overview of tachyarrhythmias, including:
- Definitions of tachyarrhythmias as disturbances in heart rhythm over 100 beats per minute.
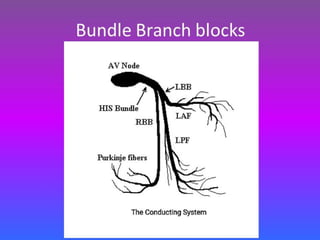
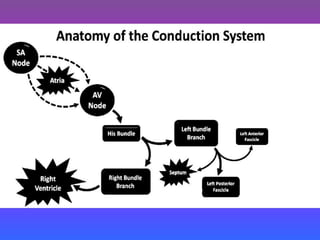
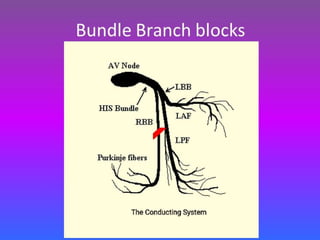
- Anatomy and electrophysiology of the heart's conduction system.
- Mechanisms of arrhythmogenesis including disorders of impulse formation and conduction.
- Diagnostic approach involving history, physical exam, ECGs, monitoring, and invasive studies.
- Treatment modalities including antiarrhythmic drugs and ablation procedures for various specific arrhythmias like atrial fibrillation, supraventricular tachycardias, and ventricular arrhythmias.WIDE QRS TACHYCARDIA
WIDE QRS TACHYCARDIAhttps://aiimsbhubaneswar.nic.in/
Ěý
1) The document defines wide complex tachycardia as a rhythm with a QRS duration ≥120ms and heart rate >100 bpm.
2) The main causes listed are ventricular tachycardia (80% of cases) and supraventricular tachycardia with aberrancy.
3) Key features that can help differentiate the underlying rhythm include QRS duration, axis, morphology, and the presence or absence of AV dissociation on electrocardiogram.Sinus tachycardia
Sinus tachycardiaAnn Bentley
Ěý
Sinus tachycardia is characterized by a heart rate over 100 beats per minute originating from the sinus node. It can be a normal response to exercise or stress or indicate underlying conditions like heart failure. Symptoms may occur if the heart rate is very fast or the patient has heart disease. Treatment involves addressing the underlying cause and reducing stress or anxiety.11.atrial flutter for basic ep.final
11.atrial flutter for basic ep.finalTaiwan Heart Rhythm Society
Ěý
Atrial flutter is a reentrant tachycardia involving the right atrium. There are two main types - typical atrial flutter which revolves counterclockwise around the tricuspid annulus, and reverse typical atrial flutter which revolves clockwise. Catheter ablation aims to create a continuous linear lesion across the cavotricuspid isthmus to block conduction and terminate the arrhythmia. Successful ablation is confirmed by the inability to induce flutter and demonstration of bidirectional conduction block across the ablation line.Premature Atrial complexes
Premature Atrial complexesMohamed Salih Aziz
Ěý
The document discusses three types of atrial premature complexes:
1. Normally conducted complexes which have an early P wave that conducts normally with a PR interval that may be normal, increased, or decreased and a QRS similar to sinus rhythm.
2. Non-conducted complexes where an early P wave is not followed by a QRS and the P wave is often hidden in the T wave.
3. Complexes with aberrant conduction where the early P wave is followed by a QRS with an abnormal conduction pattern most commonly right bundle branch block but sometimes left bundle branch block.Aortic regurgitation
Aortic regurgitationVitrag Shah
Ěý
The document discusses aortic regurgitation, including its anatomy, etiology, pathophysiology, epidemiology, clinical manifestations, diagnosis, and management. Key points include:
- Aortic regurgitation occurs when the aortic valve fails to close properly, allowing blood to flow back into the left ventricle during diastole.
- Causes include conditions like infective endocarditis, bicuspid aortic valve, hypertension, and Marfan syndrome.
- In acute severe cases, a rapid increase in left ventricular preload can cause pulmonary edema and cardiogenic shock. Chronic cases involve left ventricular dilation and hypertrophy to compensate for the increased preload over time.
- Physical exam mayVentricular tachycardia
Ventricular tachycardiaApollo Hospitals
Ěý
Ventricular tachycardia is a fast heart rhythm originating from the ventricles with a rate over 100 bpm. It is classified based on duration (sustained vs non-sustained), morphology (monomorphic, polymorphic, sinusoidal), and symptoms. Causes include structural heart disease, electrolyte abnormalities, drugs, and prolonged QT interval. Diagnosis involves ECG criteria showing ventricular origin. Treatment depends on hemodynamic stability and may include antiarrhythmic drugs, implantable cardioverter-defibrillator, catheter ablation, or surgery. Recurrent ventricular tachycardia is managed long term with devices, drugs, and treatment of underlying causes.Approach to a patient with T wave abnormality in ECG
Approach to a patient with T wave abnormality in ECGPROFESSOR DR. MD. TOUFIQUR RAHMAN
Ěý
This document discusses the fundamentals of electrocardiogram (ECG) interpretation with a focus on T-wave abnormalities, including their characteristics, clinical implications, and various conditions associated with them. It provides detailed case studies demonstrating how specific T-wave patterns relate to medical conditions like hyperkalemia, myocardial ischemia, and different cardiomyopathies. The document emphasizes the importance of recognizing these patterns for accurate diagnosis and management in cardiology.ECG- ST segment
ECG- ST segmentPROFESSOR DR. MD. TOUFIQUR RAHMAN
Ěý
This document contains a lecture on ST segment abnormalities from Professor Dr. Md Toufiqur Rahman. It discusses the normal ST segment and various causes of ST elevation and depression. ST segment abnormalities most commonly indicate myocardial ischemia or infarction. Other causes of ST elevation discussed include pericarditis, early repolarization, left bundle branch block, left ventricular hypertrophy, ventricular aneurysm, Brugada syndrome, ventricular pacing, and raised intracranial pressure. The lecture includes examples and descriptions of ST segment changes in each condition.Atrial Fibrillation
Atrial Fibrillationmeducationdotnet
Ěý
1) Atrial fibrillation is the most common cardiac arrhythmia characterized by irregular electrical activity in the atria. It increases in prevalence with age and can cause complications like heart failure, stroke, and systemic embolism.
2) Management of atrial fibrillation involves rate or rhythm control as well as long-term anticoagulation to prevent thromboembolism depending on stroke risk factors. The CHA2DS2-VASc score is used to assess this risk.
3) While antiarrhythmic drugs and cardioversion can restore normal sinus rhythm, rate control is preferred for many patients. Newer anticoagulants like dabigatran and rivarACUTE CORONARY SYNDROME FOR CRITICAL CARE
ACUTE CORONARY SYNDROME FOR CRITICAL CAREAbhinovKandur
Ěý
The document defines acute coronary syndrome (ACS) as a group of diseases including unstable angina, myocardial infarction, and sudden cardiac death. ACS is classified into STEMI, NSTEMI, or unstable angina based on ECG and cardiac biomarker findings. The diagnosis of ACS involves taking a medical history, performing an ECG, and measuring cardiac biomarkers like troponin and CK-MB. Treatment involves pain relief medications, antiplatelet drugs, anticoagulants, and sometimes revascularization through procedures like angioplasty.Catecholaminergic Polymorphic VT
Catecholaminergic Polymorphic VTdrabhishekbabbu
Ěý
This document discusses catecholaminergic polymorphic ventricular tachycardia (CPVT), a condition characterized by adrenergically mediated polymorphic ventricular arrhythmias without structural heart disease. It has a prevalence of 1 in 10,000 and mortality of up to 50% before age 20 if untreated. The gold standard for diagnosis is exercise stress testing showing exercise-induced bidirectional or polymorphic ventricular tachycardia. Treatment involves lifestyle changes, beta-blockers, flecainide, and an ICD for those with cardiac arrest or recurrent arrhythmias despite medical therapy. Genetic testing identifies mutations in RYR2 or CASQ2 genes in the majority of cases.Aortic stenosis
Aortic stenosisKalpana Gogoi
Ěý
This document discusses aortic stenosis, including its causes, symptoms, diagnosis, and treatment. It notes that aortic stenosis can be valvular, subvalvular, or supravalvular and can be caused by rheumatic fever, congenital defects, or age-related calcification. Common symptoms include chest pain, shortness of breath, fatigue, and murmurs. Diagnosis involves echocardiogram, EKG, chest X-ray and cardiac catheterization. Treatment options range from medication to manage symptoms, balloon valvuloplasty, or aortic valve replacement surgery.Ventricular tachycardia
Ventricular tachycardiaPraveen Nagula
Ěý
Ventricular tachycardia can occur due to various causes like acute myocardial infarction, chronic infarction, dilated cardiomyopathy, etc. It is classified as sustained, non-sustained, monomorphic, polymorphic, etc. based on characteristics. Diagnosis involves ECG, echocardiogram, and monitoring. Treatment depends on hemodynamic stability and includes electrical cardioversion, antiarrhythmic drugs like amiodarone, lidocaine, ablation, and ICD implantation in selected cases. Recurrence risk is high in structurally abnormal hearts and prevention involves controlling triggers, antiarrhythmics, and ICDs.Narrow QRS Tachycardia
Narrow QRS Tachycardiahttps://aiimsbhubaneswar.nic.in/
Ěý
The document discusses various types of supraventricular tachycardia (SVT), including those originating from the sinoatrial, atrial, and atrioventricular sources, along with their ECG characteristics. Specific SVT types such as inappropriate sinus tachycardia, atrial fibrillation, and atrial flutter are described in detail, along with mechanisms and abnormal findings on ECG. The importance of identifying precipitating factors and acute termination strategies for SVT is also emphasized.PSVT
PSVTDr Siva subramaniyan
Ěý
This document discusses paroxysmal supraventricular tachycardia (PSVT), which represents a subset of supraventricular tachycardias (SVTs) characterized by abrupt onset and termination of a regular, rapid tachycardia. The main types of PSVT are atrioventricular nodal reentrant tachycardia (AVNRT) and atrioventricular reentrant tachycardia (AVRT) involving an accessory pathway. The document provides details on the mechanisms, clinical presentations, evaluations and management of these arrhythmias. Vagal maneuvers and adenosine are first-line treatment options that can terminate the tachycardias by slowing conduction through the atBasic of Pre-excitation syndrome
Basic of Pre-excitation syndromeLeonardo Paskah S
Ěý
This document discusses pre-excitation syndrome, specifically Wolff-Parkinson-White (WPW) syndrome and Lown-Ganong-Levine (LGL) syndrome. It defines pre-excitation syndrome as having a short PR interval and usually an abnormal QRS complex due to an accessory pathway in the cardiac conduction system. Accessory pathways can connect different parts of the heart and have faster conduction velocities than the atrioventricular node. WPW syndrome is the most common type, affecting about 1.5 per 1000 people. Common symptoms include palpitations and chest discomfort due to paroxysmal tachyarrhythmias like atrioventricular reentrant tachycardia. Management involves catheter ablationApproach to syncope
Approach to syncopeGagan Velayudhan
Ěý
Syncope is a transient loss of consciousness due to transient global cerebral hypoperfusion. It is characterized by rapid onset, short duration, and spontaneous recovery. The most common causes are reflex-mediated syncope and orthostatic hypotension, which account for one-third of syncopal episodes. Evaluation involves detailed history taking and physical examination, including orthostatic vital signs and carotid sinus massage. Tilt table testing can be used to confirm neurogenic causes when initial evaluation is insufficient.Ecg & arrhythmias
Ecg & arrhythmiasBP KOIRALA INSTITUTE OF HELATH SCIENCS,, NEPAL
Ěý
The document discusses electrocardiograms (ECGs) and cardiac arrhythmias. It begins by explaining how the heart generates electrical currents that can be recorded as ECG tracings. It then covers ECG basics like normal sinus rhythm, heart rate calculation, and the cardiac conduction system. The document discusses various types of arrhythmias including premature beats, tachycardias, fibrillation, and heart blocks. It provides examples of ECG tracings of normal and abnormal rhythms. In summary, the document provides an overview of ECGs, how to analyze rhythms, and examples of common arrhythmias.Ventricular activation
Ventricular activationkashif Anwer
Ěý
The document discusses ventricular activation and broad complex tachycardia. It contains slides created by Dr. Mark Hall, a cardiac electrophysiologist at Liverpool Heart and Chest Hospital, on the topics of ventricular activation and broad complex tachycardia.More Related Content
What's hot (20)
tachyarrythmias d
tachyarrythmias dRavi Kanth
Ěý
This document provides an overview of tachyarrhythmias, including:
- Definitions of tachyarrhythmias as disturbances in heart rhythm over 100 beats per minute.
- Anatomy and electrophysiology of the heart's conduction system.
- Mechanisms of arrhythmogenesis including disorders of impulse formation and conduction.
- Diagnostic approach involving history, physical exam, ECGs, monitoring, and invasive studies.
- Treatment modalities including antiarrhythmic drugs and ablation procedures for various specific arrhythmias like atrial fibrillation, supraventricular tachycardias, and ventricular arrhythmias.WIDE QRS TACHYCARDIA
WIDE QRS TACHYCARDIAhttps://aiimsbhubaneswar.nic.in/
Ěý
1) The document defines wide complex tachycardia as a rhythm with a QRS duration ≥120ms and heart rate >100 bpm.
2) The main causes listed are ventricular tachycardia (80% of cases) and supraventricular tachycardia with aberrancy.
3) Key features that can help differentiate the underlying rhythm include QRS duration, axis, morphology, and the presence or absence of AV dissociation on electrocardiogram.Sinus tachycardia
Sinus tachycardiaAnn Bentley
Ěý
Sinus tachycardia is characterized by a heart rate over 100 beats per minute originating from the sinus node. It can be a normal response to exercise or stress or indicate underlying conditions like heart failure. Symptoms may occur if the heart rate is very fast or the patient has heart disease. Treatment involves addressing the underlying cause and reducing stress or anxiety.11.atrial flutter for basic ep.final
11.atrial flutter for basic ep.finalTaiwan Heart Rhythm Society
Ěý
Atrial flutter is a reentrant tachycardia involving the right atrium. There are two main types - typical atrial flutter which revolves counterclockwise around the tricuspid annulus, and reverse typical atrial flutter which revolves clockwise. Catheter ablation aims to create a continuous linear lesion across the cavotricuspid isthmus to block conduction and terminate the arrhythmia. Successful ablation is confirmed by the inability to induce flutter and demonstration of bidirectional conduction block across the ablation line.Premature Atrial complexes
Premature Atrial complexesMohamed Salih Aziz
Ěý
The document discusses three types of atrial premature complexes:
1. Normally conducted complexes which have an early P wave that conducts normally with a PR interval that may be normal, increased, or decreased and a QRS similar to sinus rhythm.
2. Non-conducted complexes where an early P wave is not followed by a QRS and the P wave is often hidden in the T wave.
3. Complexes with aberrant conduction where the early P wave is followed by a QRS with an abnormal conduction pattern most commonly right bundle branch block but sometimes left bundle branch block.Aortic regurgitation
Aortic regurgitationVitrag Shah
Ěý
The document discusses aortic regurgitation, including its anatomy, etiology, pathophysiology, epidemiology, clinical manifestations, diagnosis, and management. Key points include:
- Aortic regurgitation occurs when the aortic valve fails to close properly, allowing blood to flow back into the left ventricle during diastole.
- Causes include conditions like infective endocarditis, bicuspid aortic valve, hypertension, and Marfan syndrome.
- In acute severe cases, a rapid increase in left ventricular preload can cause pulmonary edema and cardiogenic shock. Chronic cases involve left ventricular dilation and hypertrophy to compensate for the increased preload over time.
- Physical exam mayVentricular tachycardia
Ventricular tachycardiaApollo Hospitals
Ěý
Ventricular tachycardia is a fast heart rhythm originating from the ventricles with a rate over 100 bpm. It is classified based on duration (sustained vs non-sustained), morphology (monomorphic, polymorphic, sinusoidal), and symptoms. Causes include structural heart disease, electrolyte abnormalities, drugs, and prolonged QT interval. Diagnosis involves ECG criteria showing ventricular origin. Treatment depends on hemodynamic stability and may include antiarrhythmic drugs, implantable cardioverter-defibrillator, catheter ablation, or surgery. Recurrent ventricular tachycardia is managed long term with devices, drugs, and treatment of underlying causes.Approach to a patient with T wave abnormality in ECG
Approach to a patient with T wave abnormality in ECGPROFESSOR DR. MD. TOUFIQUR RAHMAN
Ěý
This document discusses the fundamentals of electrocardiogram (ECG) interpretation with a focus on T-wave abnormalities, including their characteristics, clinical implications, and various conditions associated with them. It provides detailed case studies demonstrating how specific T-wave patterns relate to medical conditions like hyperkalemia, myocardial ischemia, and different cardiomyopathies. The document emphasizes the importance of recognizing these patterns for accurate diagnosis and management in cardiology.ECG- ST segment
ECG- ST segmentPROFESSOR DR. MD. TOUFIQUR RAHMAN
Ěý
This document contains a lecture on ST segment abnormalities from Professor Dr. Md Toufiqur Rahman. It discusses the normal ST segment and various causes of ST elevation and depression. ST segment abnormalities most commonly indicate myocardial ischemia or infarction. Other causes of ST elevation discussed include pericarditis, early repolarization, left bundle branch block, left ventricular hypertrophy, ventricular aneurysm, Brugada syndrome, ventricular pacing, and raised intracranial pressure. The lecture includes examples and descriptions of ST segment changes in each condition.Atrial Fibrillation
Atrial Fibrillationmeducationdotnet
Ěý
1) Atrial fibrillation is the most common cardiac arrhythmia characterized by irregular electrical activity in the atria. It increases in prevalence with age and can cause complications like heart failure, stroke, and systemic embolism.
2) Management of atrial fibrillation involves rate or rhythm control as well as long-term anticoagulation to prevent thromboembolism depending on stroke risk factors. The CHA2DS2-VASc score is used to assess this risk.
3) While antiarrhythmic drugs and cardioversion can restore normal sinus rhythm, rate control is preferred for many patients. Newer anticoagulants like dabigatran and rivarACUTE CORONARY SYNDROME FOR CRITICAL CARE
ACUTE CORONARY SYNDROME FOR CRITICAL CAREAbhinovKandur
Ěý
The document defines acute coronary syndrome (ACS) as a group of diseases including unstable angina, myocardial infarction, and sudden cardiac death. ACS is classified into STEMI, NSTEMI, or unstable angina based on ECG and cardiac biomarker findings. The diagnosis of ACS involves taking a medical history, performing an ECG, and measuring cardiac biomarkers like troponin and CK-MB. Treatment involves pain relief medications, antiplatelet drugs, anticoagulants, and sometimes revascularization through procedures like angioplasty.Catecholaminergic Polymorphic VT
Catecholaminergic Polymorphic VTdrabhishekbabbu
Ěý
This document discusses catecholaminergic polymorphic ventricular tachycardia (CPVT), a condition characterized by adrenergically mediated polymorphic ventricular arrhythmias without structural heart disease. It has a prevalence of 1 in 10,000 and mortality of up to 50% before age 20 if untreated. The gold standard for diagnosis is exercise stress testing showing exercise-induced bidirectional or polymorphic ventricular tachycardia. Treatment involves lifestyle changes, beta-blockers, flecainide, and an ICD for those with cardiac arrest or recurrent arrhythmias despite medical therapy. Genetic testing identifies mutations in RYR2 or CASQ2 genes in the majority of cases.Aortic stenosis
Aortic stenosisKalpana Gogoi
Ěý
This document discusses aortic stenosis, including its causes, symptoms, diagnosis, and treatment. It notes that aortic stenosis can be valvular, subvalvular, or supravalvular and can be caused by rheumatic fever, congenital defects, or age-related calcification. Common symptoms include chest pain, shortness of breath, fatigue, and murmurs. Diagnosis involves echocardiogram, EKG, chest X-ray and cardiac catheterization. Treatment options range from medication to manage symptoms, balloon valvuloplasty, or aortic valve replacement surgery.Ventricular tachycardia
Ventricular tachycardiaPraveen Nagula
Ěý
Ventricular tachycardia can occur due to various causes like acute myocardial infarction, chronic infarction, dilated cardiomyopathy, etc. It is classified as sustained, non-sustained, monomorphic, polymorphic, etc. based on characteristics. Diagnosis involves ECG, echocardiogram, and monitoring. Treatment depends on hemodynamic stability and includes electrical cardioversion, antiarrhythmic drugs like amiodarone, lidocaine, ablation, and ICD implantation in selected cases. Recurrence risk is high in structurally abnormal hearts and prevention involves controlling triggers, antiarrhythmics, and ICDs.Narrow QRS Tachycardia
Narrow QRS Tachycardiahttps://aiimsbhubaneswar.nic.in/
Ěý
The document discusses various types of supraventricular tachycardia (SVT), including those originating from the sinoatrial, atrial, and atrioventricular sources, along with their ECG characteristics. Specific SVT types such as inappropriate sinus tachycardia, atrial fibrillation, and atrial flutter are described in detail, along with mechanisms and abnormal findings on ECG. The importance of identifying precipitating factors and acute termination strategies for SVT is also emphasized.PSVT
PSVTDr Siva subramaniyan
Ěý
This document discusses paroxysmal supraventricular tachycardia (PSVT), which represents a subset of supraventricular tachycardias (SVTs) characterized by abrupt onset and termination of a regular, rapid tachycardia. The main types of PSVT are atrioventricular nodal reentrant tachycardia (AVNRT) and atrioventricular reentrant tachycardia (AVRT) involving an accessory pathway. The document provides details on the mechanisms, clinical presentations, evaluations and management of these arrhythmias. Vagal maneuvers and adenosine are first-line treatment options that can terminate the tachycardias by slowing conduction through the atBasic of Pre-excitation syndrome
Basic of Pre-excitation syndromeLeonardo Paskah S
Ěý
This document discusses pre-excitation syndrome, specifically Wolff-Parkinson-White (WPW) syndrome and Lown-Ganong-Levine (LGL) syndrome. It defines pre-excitation syndrome as having a short PR interval and usually an abnormal QRS complex due to an accessory pathway in the cardiac conduction system. Accessory pathways can connect different parts of the heart and have faster conduction velocities than the atrioventricular node. WPW syndrome is the most common type, affecting about 1.5 per 1000 people. Common symptoms include palpitations and chest discomfort due to paroxysmal tachyarrhythmias like atrioventricular reentrant tachycardia. Management involves catheter ablationApproach to syncope
Approach to syncopeGagan Velayudhan
Ěý
Syncope is a transient loss of consciousness due to transient global cerebral hypoperfusion. It is characterized by rapid onset, short duration, and spontaneous recovery. The most common causes are reflex-mediated syncope and orthostatic hypotension, which account for one-third of syncopal episodes. Evaluation involves detailed history taking and physical examination, including orthostatic vital signs and carotid sinus massage. Tilt table testing can be used to confirm neurogenic causes when initial evaluation is insufficient.Ecg & arrhythmias
Ecg & arrhythmiasBP KOIRALA INSTITUTE OF HELATH SCIENCS,, NEPAL
Ěý
The document discusses electrocardiograms (ECGs) and cardiac arrhythmias. It begins by explaining how the heart generates electrical currents that can be recorded as ECG tracings. It then covers ECG basics like normal sinus rhythm, heart rate calculation, and the cardiac conduction system. The document discusses various types of arrhythmias including premature beats, tachycardias, fibrillation, and heart blocks. It provides examples of ECG tracings of normal and abnormal rhythms. In summary, the document provides an overview of ECGs, how to analyze rhythms, and examples of common arrhythmias.More from kashif Anwer (20)
Ventricular activation
Ventricular activationkashif Anwer
Ěý
The document discusses ventricular activation and broad complex tachycardia. It contains slides created by Dr. Mark Hall, a cardiac electrophysiologist at Liverpool Heart and Chest Hospital, on the topics of ventricular activation and broad complex tachycardia.Normal values of tte
Normal values of ttekashif Anwer
Ěý
- The document provides reference values and guidelines for interpreting various measurements obtained from transthoracic echocardiography (TTE) exams. It includes sections on the left ventricle, right ventricle, atria, valves, and other cardiac structures.
- Threshold values are given to define the severity of abnormalities as mild, moderate, or severe for conditions like left ventricular dysfunction, valvular diseases, and cardiac chamber enlargement.
- Recommendations from clinical guidelines are referenced to establish standard criteria for evaluating features on TTE like aortic stenosis severity based on velocities, gradients, and valve areas.M mode echocardiography
M mode echocardiographykashif Anwer
Ěý
M-mode echocardiography uses rapid sampling of a region to create sequential parallel data lines, producing continuous horizontal lines representing points of brightness. This allows visualization of motion patterns over distance and time. Measurements of structures like the mitral valve can assess morphology, movement, velocity, and timing of cardiac events. Findings include increased wall thickness, reduced valve excursion, and fluttering indicating conditions like hypertrophy, stenosis, and regurgitation.Blood vessels the aorta and its branches,
Blood vessels the aorta and its branches,kashif Anwer
Ěý
This document provides an overview and step-by-step instructions for performing an abdominal ultrasound to visualize the aorta and vena cava. It describes how to obtain transverse and longitudinal views of the vessels, identify their pulsations and relationship to nearby organs like the liver and diaphragm. The document also discusses evaluating the vessel walls, identifying branches, and measuring aneurysms for progression. Its goal is to guide ultrasonographers in thoroughly scanning the abdominal blood vessels.Measuring talent
Measuring talentkashif Anwer
Ěý
This document discusses measuring talent in organizations. It recommends using three metrics: return on investment (ROI) on manpower to evaluate costs versus profits from employees; revenue per employee to assess productivity; and workforce innovation index to gauge revenue from employee-suggested innovations. Tracking these metrics over time can help ensure a skilled workforce and identify areas needing improvement.Career limiting moves
Career limiting moveskashif Anwer
Ěý
This document lists career limiting moves that should be avoided, including loose talk, indiscipline, insincerity, being money-minded, dishonesty, arrogance, engaging in office politics, emotional outbursts, and inappropriate appearance. It provides a brief list of behaviors that could negatively impact one's career if not managed properly.Mistakes to avoid while starting a new business
Mistakes to avoid while starting a new businesskashif Anwer
Ěý
The document discusses common mistakes entrepreneurs make when starting a new business and provides advice to avoid them. It identifies mistakes like not properly evaluating ideas, inadequate planning, using the wrong business structure, frivolous spending, hiring unqualified people, poor marketing, relying on pretense, and ignoring legal/financial issues. The author advises entrepreneurs to thoroughly research and plan their business, hire the right people, focus spending on essentials, develop a strong marketing strategy, be transparent, and address any legal/financial problems promptly.Uyuni salt lake
Uyuni salt lakekashif Anwer
Ěý
The Uyuni salt lake in Bolivia is the largest salt flat in the world, covering 12,000 square kilometers at an elevation of 3,650 meters. When filled with water after rain, it becomes the world's largest mirror. Comprised of 11 layers of salt up to 10 meters deep, with a maximum depth of 120 meters, it contains an estimated 10 billion tons of salt, of which 25,000 tons are extracted each year through evaporation.Secrets of Nations
Secrets of Nationskashif Anwer
Ěý
The document summarizes that the difference between poor and rich nations is not due to factors like the age of the nation, availability of natural resources, or intellectual abilities of people. Rather, the key difference lies in the attitudes and principles followed by most citizens of each country. Rich countries became prosperous because their people generally abide by principles like ethics, integrity, responsibility, respect for laws, work ethic, savings, productivity, and punctuality. In poor countries, only a small minority follow these basic principles in their daily lives. The document argues that countries will remain poor if their people lack the will to adopt and teach the attitudes of successful societies.Building trust essential.........
Building trust essential.........kashif Anwer
Ěý
Building trust is essential to furthering one's career. Trust is gained by being open and sharing information frankly, being receptive to others' ideas, keeping commitments, having solid work to back up statements, avoiding gossip, admitting mistakes, asking for and acting on feedback, and keeping information confidential when requested. Losing trust is easy but regaining it is difficult, so following these tips can help one build and maintain trust at work.How to handle criticism
How to handle criticismkashif Anwer
Ěý
Handle criticism by acknowledging any mistakes, taking corrective action, and acknowledging the other person's motives. If the criticism is valid, take full responsibility without making excuses. After listening fully, express eagerness to improve and describe actions to address the issue. Thank the person for the feedback and acknowledge their input is valuable for helping you improve, while also stating you are open to future feedback.Kidney Stone
Kidney Stonekashif Anwer
Ěý
Kidney stones form when crystals separate from urine and stick together inside the kidney or urinary tract. They can cause severe pain and blood in the urine. Risk factors include dehydration, family history, and medical conditions. Symptoms include intense pain in the back or side and blood in the urine. Diagnosis is usually done with a CT scan. Small stones often pass on their own but larger ones may require lithotripsy or surgery to break up the stones. Drinking plenty of water can help prevent kidney stones from forming.Kidney stone
Kidney stonekashif Anwer
Ěý
Kidney stones form when crystals separate from urine and stick together inside the kidney or urinary tract. They can cause severe pain and blood in the urine. Risk factors include dehydration, family history, and medical conditions. Symptoms include intense pain in the back or side and blood in the urine. Diagnosis is usually done with a CT scan. Small stones often pass on their own but larger ones may require lithotripsy or surgery to break up the stones. Drinking plenty of water can help prevent kidney stones from forming.09 steps to achieve your goal
09 steps to achieve your goalkashif Anwer
Ěý
This document outlines 9 steps to achieve your goals: 1) Define your specific, achievable goal; 2) Set a deadline; 3) Identify your underlying purpose; 4) Recognize the benefits; 5) Instill self-belief through affirmations and visualization; 6) Identify potential obstacles; 7) Seek solutions to overcome obstacles; 8) Practice visualizing achieving your goal; 9) Create a step-by-step action plan with milestones and tasks. Taking these steps will help you stay focused and motivated to turn your dreams into a reality.How to argue?
How to argue?kashif Anwer
Ěý
Stay calm, keep a steady tone of voice, and avoid insults when arguing. Listen respectfully to the other perspective without taking small comments personally. Aim to find reasonable solutions, not get everything you want. Keep arguments brief and allow each side to speak before setting healthy boundaries if needed.An excellent theory
An excellent theorykashif Anwer
Ěý
This short document promotes the value of knowledge and learning throughout one's life. It states that "Nothing but KNOWLEDGE has The Value" and encourages us to "Keep Learning, until Our Last Breath," suggesting we should continuously seek knowledge even at the end of our lives. The overall message is that knowledge is extremely valuable.Ad
Recently uploaded (20)
Navigating the Open Enrollment Period for Medicare Supplement Insurance in Sa...
Navigating the Open Enrollment Period for Medicare Supplement Insurance in Sa...dfwdirectinsurance
Ěý
Understanding Medicare options can feel like navigating a maze, especially during the open enrollment period. For residents of Sarasota approaching age 65 or already enrolled in Medicare, this window offers a vital opportunity to secure additional health coverage that helps reduce out-of-pocket costs. If you're planning to enhance your Medicare plan, it's essential to understand the rules, deadlines, and options that apply to Medicare supplement insurance in Sarasota.Drmohamedaslam_resident_copd2025_fm.pptx
Drmohamedaslam_resident_copd2025_fm.pptxAslam
Ěý
COPD :LATEST GUIDELINES 2025
REFERENCE: Harrison’s Principles of Internal Medicine
GOLD -2025 Guidelines
It highlights updated diagnostic criteria, pharmacological and non-pharmacological treatment options, and current best practices for resident doctors and healthcare professionals.
Ideal for medical students, residents, and practitioners seeking an up-to-date, evidence-based reference.
👉 Download, share, and feel free to reach out for related study material!From Preservation To Regeneration--The Stem Cell Era of Hair Restoration_DrAl...
From Preservation To Regeneration--The Stem Cell Era of Hair Restoration_DrAl...Alan Bauman
Ěý
How can the latest in Regenerative Medicine help those suffering from hair loss? Cell Surgical Conference 2025 featured Dr Alan Bauman as a faculty member once again to discuss all things related to hair loss, hair transplantation and the use of regenerative stem cell therapies for hair restoration. Severe Acute Respiratory Syndrome (SARS)
Severe Acute Respiratory Syndrome (SARS)Dr. Anu Marhatta
Ěý
This slide is for educational purposes only. ELECTROMYOGRAPHY.pptX by GOKULAKRISHNAN.
ELECTROMYOGRAPHY.pptX by GOKULAKRISHNAN.GOKULAKRISHNAN JANARTHANAN
Ěý
Electromyography is basically the study of motor unit activity.
In electromyography, the study of the electrical activity of contracting muscle provides information concerning the structure and function of the motor units.
Quality by Design Tools in Pharmaceutical Manufacturing Technology
Quality by Design Tools in Pharmaceutical Manufacturing Technology39KomalZaveri
Ěý
In Qbd why risk assessment needed that explained
Design Space and DoE relationship with each other.
OUR SRS SBRT EXPERIENCE BY DR KANHU CHARAN PATRO
OUR SRS SBRT EXPERIENCE BY DR KANHU CHARAN PATROKanhu Charan
Ěý
OUR SRS SBRT EXPERIENCE BY DR KANHU CHARAN PATROSelf-Awareness and Self-Care How Professionals Can Avoid Burnout
Self-Awareness and Self-Care How Professionals Can Avoid BurnoutOlaf Kraus de Camargo
Ěý
Closing Keynote at the IV OGĂ“LNOPOLSKA KONFERENCJA & WARSZTATY
KomunikAACja, Samoswiadomosc, Seksualnosc
June 13th – 14th, 2025
An overview of the definition and presentation of burnout in healthcare workers, strategies to prevent it and to build resilience. The presentation also explores the barriers and enablers to introducing wellness strategies in organizations.An interesting case of facial Swelling in an autoimmune rheumatic disease Ahm...
An interesting case of facial Swelling in an autoimmune rheumatic disease Ahm...Internal medicine department, faculty of Medicine Beni-Suef University Egypt
Ěý
An interesting case of facial Swelling in an autoimmune rheumatic disease Ahmed Yehia EGYSIR Conference Yoga Postures to Practice
for Holistic (Physical, Mental, and Cognitive) Well...
Yoga Postures to Practice
for Holistic (Physical, Mental, and Cognitive) Well...Bhoj Raj Singh
Ěý
An ancient System for holistic health (mental and physical) and wellbeing, is a scientific art of living with harmony (connecting) of mind and body. Although much more ancient than Patanjali, who documented yoga systematically about 2000 years ago, Patanjali is often referred to as the "father of modern yoga."
Yoga postures are commonly depicted in ancient paintings, carvings, and sculptures in almost all civilizations and religions, thus Yoga can’t be described as an act of Hinduism. It originated long before any religion on Earth, with the emergence of life on the Planet. All yoga poses are natural, and what is not natural is not yoga; it isĚýViyoga.
Besides Vedic Yoga, Hatha, Vinyasa, Ashtanga, Iyengar, Yin, Restorative, Kundalini, Bikram, Sahaj, and Power yoga are some popular types.
VinyasaĚýYoga is the closest form to Vedic Yoga; it is known for its flowing movements, not very rigorous, not too much straining, actions flow with the breath.
Though all yoga may lead to meditation (Dhyan) for your inner upliftment, it is not the same as described in Hinduism for self-liberation.
In Hinduism, different paths of life looking distinct but can be practiced all together, they are: Karma Yoga (selfless action and service), Bhakti Yoga (devotion and love for God or Godly power), Jnana (Gyan) Yoga (gaining knowledge for self-realization through wisdom), Dhyan Yoga (meditation) and Kriya Yoga (optimum utilization of your vital and muscular energy).Ěý
Bias, Cofounding Bias, Matching , Blinding
Bias, Cofounding Bias, Matching , BlindingDr. Anu Marhatta
Ěý
The slide contains small sippets about the bias, confounding bias, and the ways by which we can remove them. Like by using the methods such as matching and blinding. This slide can be useful as a reference for students in MBBS. Design of cosmeceuticals products;sunprotection,sunscreens
Design of cosmeceuticals products;sunprotection,sunscreensSwami ramanand teerth marathwada university
Ěý
Design of cosmeceuticals products and improving the skin to protection sun burning, used sunscreens, sunprotections Aspirin powder or Acetyl salicylic acid powder.docx
Aspirin powder or Acetyl salicylic acid powder.docxkopalsharma85
Ěý
pharmacy exercise on aspirin powderTuberculosis Nepal 2025 National Plan.pptx
Tuberculosis Nepal 2025 National Plan.pptxDr. Anu Marhatta
Ěý
The presentation contains preventive therapy, the DOTS program, and the national program of Nepal. This material is intended for educational purposes only.From Wheals to Wellness: Transforming Chronic Spontaneous Urticaria Care With...
From Wheals to Wellness: Transforming Chronic Spontaneous Urticaria Care With...PVI, PeerView Institute for Medical Education
Ěý
Chair, Michael E. Manning, MD, FAAAAI, FACAAI, discusses chronic spontaneous urticaria in this CME activity titled “From Wheals to Wellness: Transforming Chronic Spontaneous Urticaria Care With Emerging Solutions.” For the full presentation, downloadable Practice Aids, and complete CME information, and to apply for credit, please visit us at . CME credit will be available until June 11, 2026.nanoparticle and liposomes ppt .(NTDS)pdf
nanoparticle and liposomes ppt .(NTDS)pdfsiddhikalbande
Ěý
Nanoparticles and liposomes are advanced carriers used for targeted drug delivery.
Nanoparticles enhance drug effectiveness by directing treatment to specific sites.
Liposomes are biocompatible vesicles that enable controlled and sustained drug release.COUGH AND THIER DRUGS AND MODE OF ACTION.pptx
COUGH AND THIER DRUGS AND MODE OF ACTION.pptxPackialakshmiP
Ěý
COUGH AND THIER DRUGS AND MODE OF ACTIONNavigating the Open Enrollment Period for Medicare Supplement Insurance in Sa...
Navigating the Open Enrollment Period for Medicare Supplement Insurance in Sa...dfwdirectinsurance
Ěý
An interesting case of facial Swelling in an autoimmune rheumatic disease Ahm...
An interesting case of facial Swelling in an autoimmune rheumatic disease Ahm...Internal medicine department, faculty of Medicine Beni-Suef University Egypt
Ěý
Design of cosmeceuticals products;sunprotection,sunscreens
Design of cosmeceuticals products;sunprotection,sunscreensSwami ramanand teerth marathwada university
Ěý
From Wheals to Wellness: Transforming Chronic Spontaneous Urticaria Care With...
From Wheals to Wellness: Transforming Chronic Spontaneous Urticaria Care With...PVI, PeerView Institute for Medical Education
Ěý
Ad