



















Meningitis case presentation
- 1. CASE PRESENTATION ON ACUTE MENINGITIS PRESENTED BY: B.ROSHITHA V PHARM.D 13P91T0020
- 2. PATIENT DEMOGRAPHIC DETAILS: Patient Name : Miss.x Age : 14years Gender : Female Ward : Pediatrics OP No : ----- Date of Admission : 26-06-2017 Date of discharge :30-07-2017 Informant : Mother Address : ---
- 3. Chief Complaints: 1. Persistant headache since 2 months, 2. On and off fever since 1 month, 3. Cough and cold since 1 week. History of present illness: 14 years female child presented with the complaints of high grade, on and off, intermittent fever since one month and cough and cold since 1 week. headache since 2 months in frontotemporal region, H/O breathlessness, eye discharge and redness of eyes present.
- 4. Past history: No history of similar complaints. Treatment history: Taken treatment for fever in locally located hospitals. General examination: Pallor : positive Jaundice : Negative Clubbing : Negative Cyanosis : Negative Pedal edema : Negative Lymphadenopathy : Negative Head to toe examination : Within normal limits
- 5. Physical examination: 1) Vitals: Heart rate : 104 beats/min Respiratory rate : 38/mim Blood pressure : 90/60 mm of hg Temperature : 101’é░ F 2) Systemic examination: Cvs: Normal RS: B/L NVBS+ B/L creps+ve P/A: Soft, non tender CNS: Headache in frontotemporal region, neck pain (non significant), no meningial signs.
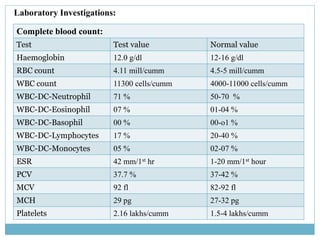
- 6. Laboratory Investigations: Complete blood count: Test Test value Normal value Haemoglobin 12.0 g/dl 12-16 g/dl RBC count 4.11 mill/cumm 4.5-5 mill/cumm WBC count 11300 cells/cumm 4000-11000 cells/cumm WBC-DC-Neutrophil 71 % 50-70 % WBC-DC-Eosinophil 07 % 01-04 % WBC-DC-Basophil 00 % 00-o1 % WBC-DC-Lymphocytes 17 % 20-40 % WBC-DC-Monocytes 05 % 02-07 % ESR 42 mm/1st hr 1-20 mm/1st hour PCV 37.7 % 37-42 % MCV 92 fl 82-92 fl MCH 29 pg 27-32 pg Platelets 2.16 lakhs/cumm 1.5-4 lakhs/cumm
- 7. Serum creatinine 0.45 mg/dl 0.30-130 mg/dl Serum urea 16 mg/dl 10.00-40.00 mg/dl Lumbar pucture test: CSF Glucose 51 mg/dl 40-80 mg/dl CSF Protien 23 mg/dl 10-40 mg/dl CSF Total count 15 cells/cumm 0-8 cells/cumm CSF DC Lymphocytes 12 cells/cumm - CSF DC Neutrophils 03 cells/cumm - CSF RBC 115 cells/cum Nill Urine analysis: Urine albumin Nill Nill Urine sugar Nill Nill Pus cells 1-2 / hpf 1-2 /hpf Epithelial cells 1-2 /hpf 1-2 /hpf RBC Nill /hpf Nill
- 8. Other diagnostic tests: ŌĆó MRI scan - MRI scan has noted minimal diffuse leptomeningial enhancement which may implicate meningitis. ŌĆó CT scan - Right maxillary sinusitis and ethmoidal sinusitis. ŌĆó PCR M.Tuberculosis - Negative Confirmatory diagnosis: Acute meningitis and acute conjuctivitis.
- 9. ’éŚ SUBJECTIVE: A 14years old female patient was admitted in the department of pediatrics with complaints of of high grade, on and off, intermittent fever since one month and cough and cold since 1 week. headache since 2 months in fronto temporal region, breathlessness, eye discharge and redness of eyes present. ’éŚ OBJECTIVE: On examination the patient was conscious and febrile. The patient has headache in fronto temporal region, neck pain, right eye swelling, redness,and watery discharge from both eyes. Laboratory investigations revealed that she has an increased ESR rate (42mm/1st hr) and increased CSF total count(15 cells/cumm). MRI scan has noted minimal diffuse leptomeningial enhancement which may implicate meningitis. ’éŚ ASSESSMENT: Based on subjective and objective evaluation the patient was diagnosed with ŌĆ£Acute Meningitis and Acute ConjuctivitisŌĆØ and the treatment is as follows SOAP NOTES:
- 10. DRUG NAME INDICATI ON DOSE R.O.A FEQUE NCY STARTI NG DATE ENDIN G DATE Moxicip drops (Moxifloxocin) Antibiotic 0.5% W/V 2 drops occular QID 26-06-17 30-06-17 Inj.ceftriaxone Antibiotic 1g IV BD 26-06-17 27-06-17 Inj.Amikacin Antibiotic 180mg IV BD 26-06-17 09-07-17 T.Paracetamol Antipyretic 500mg oral QID 26-06-17 08-07-17 Otrivin nasal drops (Xylometazoline) Decongestan t 2 drops nasal QID 26-06-17 07-07-17 Inj.piptaz (piperacillin tazobactum) Antibiotic 2.5mg IV TID 26-06-17 07-07-17
- 11. DRUG NAME INDICATI ON DOSE R.O.A FEQUE NCY STARTI NG DATE ENDIN G DATE Refresh tear drops (CMC sodium) Occular lubricant 2 drops occular QID 26-06-17 03-07-17 FML-T eye drops (flourometholone+ Tobramycin) Gluco corticoid+ antibiotic 1 drop occular QID 26-06-17 03-07-17 Inj.pantop (pantoprazole) Proton pump inhibitor 40mg IV OD 02-07-17 04-07-17 Inj.diclofenac NSAID 75mg/ 3ml IM OD 02-07-17 02-07-17 T.Combiflam (ibuprofen+ paracetamol) NSAID ┬Į tab (400+ 325 mg) Oral SOS 02-07-12 02-07-17 Inj.mannitol Osmotic diuretic 50ml IV BD 08-07-17 09-07-17
- 12. BRAND NAME GENERIC NAME INDICATI ON DOSE R.O.A FEQUE NCY STARTI NG DATE ENDIN G DATE T.Noxdom (Domperidone) Anti emetic 250mg oral BD 08-07-17 24-07-17 Syp.glycerol To releive pressure in brain 10ml oral TID 09-07-17 23-07-17 Inj.vancomycin Antibiotic 400mg IV QID 09-07-17 23-07-17 Inj.meropenam Antibiotic 1g IV TID 09-07-17 23-07-17 T.pantop PPI 40mg oral OD 17-07-17 24-07-17 Syp.lactulose Laxtive 10ml oral BD 17-07-17 18-07-17
- 13. DRUG NAME INDICATI ON DOSE R.O.A FEQUE NCY STARTI NG DATE ENDIN G DATE Nasivion pediatrics nasal drops (oxymetazolic) decongestant 2 drops nasal TID 18-07-17 21-07-17 T.Avil (pheniramine) pheniramine 4mg oral OD 21-07-17 22-07-17
- 14. ’éŚ DAY-1(26-06-2017) Patient complaints: Fever, headache, ocasional vomiting, neck pain, redness of eyes and watery discharge from both eyes On examination : Child is conscious and febrile HR - 94/min RR - 24/min CRT - <3SEC BP - 90/60mm of hg CVS - S1S2 positive RS - B/L air entry positive CNS - Neck pain positive PLAN:
- 15. Adviced tests: Complete blood count MP(QBC) Urine analysis Ct scan MRI scan Lumbar puncture test-CSF analysis Treatment: 1) IVF ┬Į DNS+KCL 35ml/hr 2) Inj.ceftriaxone 1g IV BD 3) Inj.Amikacin 180mg IV BD 4) T.paracetamol 500mg oral QID 5) Moxicip drops 2drops occular TID 6) Otrivin nasal drops 2 drops nasal TID PHARMACEUTICAL CARE ISSUES: The given therapy was rational. No drug interactions and ADRŌĆÖS were found.
- 16. DAY-2: (27-06-2017) Patient complaints : Fever spikes. On examination : Child was conscious and febrile (101’é░F) Lab reports has revealed that the patient has acute meningitis and physical examination acute conjuctivitis was confirmed. Treatment : Patient condition was improved so same medications were continued And adviced to take steam inhalation with plain water. DAY-3: (28-06-2017) Patient complaints : Headache On examination : Chid was afebrile Treatment : Inj.cefrtiaxone was removed and inj.piptaz was added to the above therapy. Inj.piptaz 2.5mg IV BD
- 17. DAY-4 TO DAY-5: (29-06-2017 to 30-06-2017) Patient complaints: eye redness and watery discahrge On examination : The child is active and has acute conjuctivitis Treatment :To the above therapy the following medications were added Refresh tear drops 2 drops occular QID (CMC sodium) FML-T eye drops 1 drop occular QID (flourometholone+ Tobramycin) DAY6-DAY10 : (01-07-2017 to 05-07-2017) Patient complaints : no complaints On examination : the child is active and all the vitals are stable Treatment : The patient condition was improved so same therapy was continued.
- 18. DAY 11: (06-07-2017) Patient complaints :Severe headache and fever since 4am On examination : The child is dull and febrile Treatment : T.paracetamol was removed and Inj.diclofenac, Inj.pantop and T.combiflam were added Inj.diclofenac 1ml IM stat Inj.pantop 20mg IV stat OD T.Combiflam 1/2tab SOS
- 19. DAY 12-DAY 14: (07-07-2017 to 09-07-2017) Patient complaints : on and off headache and vomitings On examination : The child is concious and the BP was increased , kernigŌĆÖs sign positive, BrudzinskiŌĆÖs sign positive Treatment : Inj.diclofenac and T.combiflam and eye drops was removed.Inj.mannitol,syp.glycerol, T.Noxdom, inj.vancomycin and Inj.meropenam were added to the therapy. Inj.mannitol 50ml IV BD syp.glycerol 10ml oral TID T.Noxdom 250mg oral BD Pharmaceutical Care issues : Increased blood pressure and vomitings was observed as a side effect of Inj.diclofenac.
- 20. Inj.vancomycin 400mg IV QID Inj.meropenam 1gm IV TID DAY 15-DAY 21: (10-07-2017 to 16-07-2017) Patient complaints : no complaints On examination : child is conscious and taking feeds orally. Treatment : Patient condition was improved so same therapy was continued. DAY 22- DAY 23: (17-07-2017 to 18-07-2017) Patient complaints : constipation On examination : child is conscious and taking feeds orally. Treatment : inj.pantop was replaced with T.pantop and syp.laculose was added to the therapy. syp.lactulose 10ml oral BD Pharmaceutical Care issues : constipation was observed as a side effect of meropenam.
- 21. DAY 24-DAY 26: (19-072017 to 21-07-2017) Patient complaints : 1 episode of vomiting On examination : Child is conscious and taking feeds orally. Treatment : Syp.lactulose was removed and same therapy was continued DAY 27: (22-07-2017) Patient complaints : Rashes On examination : Child is conscious and taking feeds orally. Treatment : Along with the above therapy T.avil was added T.Avil 4mg oral OD (at night) Pharmaceutical care Issues : Rashes was observed as a side effect of Inj.vancomycin
- 22. DAY 28-29: (23-07-2017 to 24-07-2017) Patient complaints : no complaints On examination : all the warning signs of meningitis was subsided and vitals was stable. Treatment : Inj.vancomycin, Inj.meropenam, syp.glycerol, T.pantop T.avil, nasivion nasal drops were stopped and T.noxdom and pantop were continued. T.noxdom 250mg oral BD T.pantop 40mg oral OD DAY-30: (30-07-2017) The patient was discharged with the following medications T. Paracetamol 500mg oral sos
- 23. PATIENT COUNSELLING: REGARDING DISEASE: ’éŚ Meningitis is an inflammation of the meninges which are protective membranes surrounding the brain and spinal cord. ’éŚ Common causes of meningitis may include bacteria,virus,fungi and parasites. REGARDING LIFE STYLE MODIFICATIONS: ’éŚ meningitis patients should consume unrestricted quantities of fresh, organic fruits and vegetables because Fruits and vegetables are known to provide antioxidants, essential fatty acids, vitamins, minerals and other nutrients that can help them heal quickly. They also strengthen the immune system that serves as the bodyŌĆÖs defense against diseases.
- 24. ’éŚ Include organic pasture-raised chicken and lean meats into your diet as well. High-quality proteins can provide you with important nutrients and vitamins such as omega-3 fats, conjugated linoleic acid (CLA) and vitamin E.4 ’éŚ Make sure you acquire these foods from trustworthy organic sources instead of sources that use confined animal feeding operations (CAFOs), so you significantly lower your risk of exposure to bacteria and artificial ingredients. ’éŚ DonŌĆÖt forget to drink adequate amounts of fluids, especially water, to help in flushing out toxins from your body. You could also drink juices made from lemons, pineapples and oranges, provided that you consume them in moderation to avoid a fructose spike. Make these drinks at home instead of buying commercially prepared varieties that are loaded with artificial sweeteners and other synthetic ingredients.
- 25. ’éŚ Avoid eating foods loaded with salt, a primary source of sodium. This is because too much salt can increase your blood pressure and cause vasoconstriction or narrowing of the arteries. Having high amounts of sodium in your system can still lead to unwanted complications.