























































Oprtic1.nerve sheath
- 1. Optic Nerve Sheath Diameter ( ONSD ) in Increased intracnial Pressures ( ICP ) A new tool in the Ultrasound Era
- 2. Causes of ICP •Obstruction CSF flow and/or  Mass effect: •Hydrocephalus absorption :  Malignancy •Extensive meningeal disease (e.g., infectious,  CVA with edema  Cerebral contusions carcinomatous,  subdural or epidural hematoma • granulomatous )  abscess Superior sagittal sinus (decreased absorption)  Diffuse Encephalopathies:  Acute liver failure •Increased CSF production :  Hypertensive Encephalopthy • Meningitis  High Altitude cerebral edema •Subarachnoid hemorrhage,  Uremic Encephalopathy  PseudotumorCerebri
- 3. Why look at ONSD?  How do we currently assess EICP :  Non-specific signs and symptoms  Imaging CT scan/MRI  Pulsatliity index  Invasive monitoring  Papilledema
- 4. CT and ICP  Moving patients  Repeat for head CT  one third of trauma need repeat head CT looking for ICP . Radiographic delay?  Initial head CTs of 100 head injured trauma patients evaluated by group of 12 radiologists :  Sensitivity 83% , Specifity 78%
- 5. Invasive ICP measurments  Gold standard External Ventricular Device  Comlipcated/ invasive procedure  Risks  Infection, parenchymal injury , bleeding  Bleeding diasthesis
- 7. Gold standard for ICP External Ventricular Device ( EVD )
- 8. Papilledema  Operator dependant  Delayed manifestation: - 24 hrs  May persist for several days to weeks after treatment
- 9. Papilledema ? Both are Normal
- 11. Outline  Basic anatomy of the Optic nerve and it’s sheath  How to measure ONSD?  Rationale and evidence for using the ONSD for Increased intracerebral pressure ( ICP )  Uses and rationale in different clinical settings :  ESRD , ESLD ,HTN crises and altitude sickness
- 12. ONSD basic anatomy  Optic Nerve:  White matter tract direct extension of the CNS surrounded by CSF  Sensitive to changes to CSF flow and intracerebral pressures ( ICP )
- 13. Intra-orbital CSF h Intracranial CSF
- 14. Optic Nerve
- 15. ONSD history  British opthalmologistHayreh  The mechanism of papiledema from increased ICP  Placed inflatable balloons in the brain of monkeys
- 19. Rapid response ONSD  Hansen et al :  Infused NS into CSF  Changes in ONSD occurred within minutes  Mean change of 1.97mm or around 83% increase  Relieving pressure  rapid decrease in size  Exception was with prolonged exposure to very high pressures showed a delay in regression Changes in ONSD mimics changes in ICP Acta Ophthalmol. 2011 Sep;89(6):e528-32.
- 20. How do we measure the ONSD?  3-7.5Mhz Probe  Supine position at around 20 degrees phlebotactic axis  Perpendicular axis at 3mm behind ON entry point  2 reading on each eye  Probe applied directly over the eyelid  Cutoff 5mm or 5.7mm
- 21. 3mm ONSD
- 22. 3mm ONSD
- 23. Lens Vitreous A-A 0.3cm B-B 0.62 cm
- 24. ONSD False Positive  Emerg Med J 2007;24:251–254. doi: 10.1136/emj.2006.040931 Volume status Emerg Med J 2007;24:251–254. doi: 10.1136/emj.2006.040931 Abdullah SadikGirisgin, ErdalKalkan, SedatKocak, BasarCander, MehmetGul, Mustafa Semiz
- 25. Reproducible results  54 patients:  28 confirmed EICP via CT scan  26 no evidence of EICP
- 27. ONSD evidence based approach  Most studies  Trauma or neurosurgical patients  3 major studies on ONSD ( briefly )
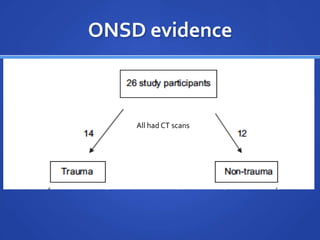
- 28. ONSD evidence  Prospective study on 26 ED patients  ONSD cutoff > 0.5 cm All had CT scans Emer Med J published online August 15, 2010 ,Robert Major, Simon Girling and Adrian Boyleg
- 29. ± ± ≥’ÔɆ100% NPVÔɆ95% Sens 86% Sepcificity 99% for EICP ONSD cutoff >5mm
- 30. ONSD evidence  Small sample size  Non-trauma  GSC: 8  Compared to CT scan
- 31. Invasive and non-invasive comparison 76 patients Pulsatility index 26 Control 18 32 Moderate Severe Invasive ICP Moderate  Marshall score I and GSC > 8 monitoring Severe  Marshall score >I and GCS < 8
- 32. 76 patients Brain CT injury scale No CT done Normal CT Abnormal CT 18% 82% ONSD cutoff 5.7mm
- 33. Non-invasive Invasive Monitoring monitoring
- 34. ROC :0.93 Sens : 74% Spec: 99% ONSD cutoff > 5.7mm TheodorosSoldtos, Optic nerve sonography in the diagnostic Evaluation of adult brain injury, Critical care 2008;12 R 67
- 35. Prospective Blind observational trial 31 ICU patients with severe TBI GSC<8 16 EICP 15 Normal ICP All patients underwent invasive ICP monitoring Intensive Care Med (2007) 33:1704–1711, T. Geeraerts () · Y. Launey · L. Martin ·J. Pottecher · B. Vigué · J. Duranteau ·D. Benhamou
- 36. 5.7 mm
- 37. ROC: 0.96 Sens: 91% Spec: 94% Thomas Geerats M.D, Ultrasonography of Optic nerve Sheath may be useful in detecting raised ICP After head trauma. Intensive care Medicine 2007, 33:1704-1711
- 38. ONSD evidence conclusion  Cutoff> 5.7mm for EICP   Sensitivity of around 93%  Specificity: 96%  5-5.7mm  Sensitivity is maintained however Specificity declines to 83%  Screening tool  Surrogate marker for EICP
- 39. ICP causes Obstruction CSF flow and/or Diffuse Encephalopathies: absorption : ESLD ESRD •Hydrocephalus Hypertensive Encephalopthy High Altitude cerebral edema •Extensive meningeal disease granulo (e.g., infectious, carcinomatous, matous ) Mass effect: •Superior sagittal sinus (decreased •Malignancy absorption) •CVA with edema Increased CSF production : •Cerebral contusions •Meningitis •Subdural or epidural hematoma •Subarachnoid hemorrhage, •Abscess
- 40. Study  Prospective observational/descriptive analysis  Medicine patient admitted to general medicine floor , MICU ESLD / ESRD / HTN crisis  No head / ocular trauma  No other cause for EICP  Comparing ONSD diameter of non-encephalopathy v/s encephalopathy pre-treatment /24hrs post-treatment  Convenience sample
- 41. Hypothesis  Absolute value of ONSD would be high among the encephalopathic group and would normalize after treatment  Statistically significant change in ONSD pre and post treatment
- 42. Definitions  EICP: - > 20 mmHg, If invasive monitoring available .  Radiographic evidence of raised ICP as determined by CT  ONSD : cut-off of 5.7 mm to define enlarged ONSD ,  ESLD and Uremia straightforward  HTN encephalopathy ? Unclear and vague definition.
- 43. Method  7-12 MHz while patient is at 20 degree angle  2 measurements from each eye ( for a total of 4 per patient )  Measurements will be taken both prior and within 24hrs after treatment
- 44. ESLD and ICP  Fulminant hepatic failure  80% EICP  Ammonia and Manganese astrocyte edema  Chronic ESLD  EICP only in stage IV hepatic encephalopathy
- 45. N=24 No Encephalopathy Encephalopathy N=10 N=14 Stage I Stage II Stage III Stage IV N=2 N=5 N=3 N=0
- 46. Pretreament ESLD 10 •Stage I ONSD in mm 9 •Stage II 8 •Stage III 7 6 5.7mm 5 4 3 2 1 N= 14 N=10 0 Encephalopathy No Encephalopathy With Encephalopathy
- 47. Post-treament ESLD 10 •Stage I ONSD in mm 9 •Stage II 8 •Stage III 7 Relative decrease 57% 6 5.7mm 5 4 3 2 1 N= 14 N= 10 0 Encephalopathy No Encephalopathy With Encephalopathy
- 48. Summary ESLD Pretreatment Post-treatment 10 ONSD in mm 10 •Stage I 9 9 •Stage II 8 8 7 7 •Stage III 6 6 5.7mm 5 5 4 4 3 3 2 2 1 1 0 N= 8 0 N= 8 N= 14 N= 14 No Encephalopathy With No With Encephalopathy Encephalopathy Encephalopathy
- 49. ESRD and ICP  Dialysis Dysequilibrium Syndrome  Very high BUN > 110
- 50. Pretreatment ESRD Pretreatment Post-treatment 10 ONSD in mm 9 8 7 46 %decrease 63% decrease 6 5 4 3 2 N= 13 N= 4 1 No With No With 0 Encephalopathy Encephalopathy Encephalopathy Encephalopathy yes No 1/9/02
- 51. Data analysis  Relative decrease in ONSD in both groups was significant  NO encephalopathy: - 46%  With Encephalopathy: - 63%  Other etiologies for increase ONSD :  Volume status  HTN  Utility in predicting DDS?
- 52. HTN crisis  Most common manifestation are neurologic :  44% with HTN emergency have neurologic manifestations  16% HTN encephalopathy  Clinically subtle  Pathophysiology Breakthrough autoregulation  CT head to r/o CVA helpful however in HTN encephalopathy not so much
- 55. HTN crisis Pretreatment Post-treatment 10 ONSD in mm Encephalopathic 9 5.2mm 7.2mm 8 7 57% decrease 68% decrease 6 5 4 3 2 N= 11 N= 5 1 Uncontrolled HTN emergency Uncontrolled HTN emergency 0 HTN HTN yes No 1/9/02
- 56. Data analysis  Uncontrolled HTN had rather high ONSD subclinical EICP  Relative size decrease :  57% in Uncontrolled HTN  68% HTN emergency
- 57. High altitude sickness  No data yet  14er’s ONSD at base , peak , base  Symptoms of Altitude sickness  ONSD absolute value and change
- 58. Conclusion  ONSD: Reliable surrogate marker for EICP  Quick bedside evaluation that competes with CT scans  Reproducible results easy to learn  Large area of research  Downfalls: - Etiology
- 59. Thank you
Editor's Notes
- Increased popularity