GENERAL ASPECTS OF FRACTURE.pptx
Download as pptx, pdf0 likes112 views

Fractures can be classified based on their etiology, displacement, relationship to the external environment, and pattern. Traumatic fractures result from injury while pathological fractures occur through weakened bone. Stress fractures are caused by repetitive stress. Treatment involves emergency care like splinting, followed by definitive care such as closed or open reduction and immobilization. Rehabilitation aims to regain function. Complications can be immediate like shock, early like fat embolism, or late such as malunion. Proper treatment seeks to reduce fractures and preserve limb function.



GENERAL ASPECTS OF FRACTURE.pptx
- 1. GENERAL ASPECTS OF FRACTURE DR. CH RAKESH SINGHA 2ND YEAR PGT, DEPT. OF ORTHOPAEDICS SILCHAR MEDICAL COLLEGE & HOSPITAL
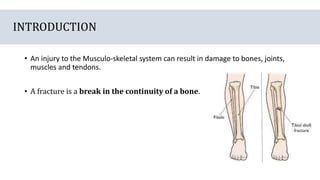
- 2. INTRODUCTION âĒ An injury to the Musculo-skeletal system can result in damage to bones, joints, muscles and tendons. âĒ A fracture is a break in the continuity of a bone.
- 4. CLASSIFICATION âĒ It can be classified on the basis of - Aetiology - The relationship of the fracture with the external environment, - The displacement of the fracture & - The pattern of the fracture.
- 5. ON THE BASIS OF AETIOLOGY 1) Traumatic fracture: - A fracture sustained due to trauma is called a traumatic fracture. - Most fractures seen in day-to-day practice fall into this category - e.g., fractures caused by a fall, - road traffic accident, - physical assault etc.
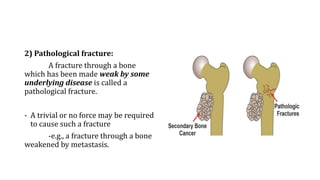
- 6. 2) Pathological fracture: A fracture through a bone which has been made weak by some underlying disease is called a pathological fracture. - A trivial or no force may be required to cause such a fracture -e.g., a fracture through a bone weakened by metastasis.
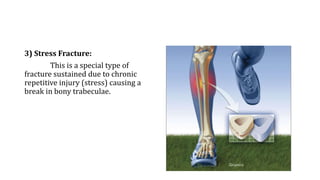
- 7. 3) Stress Fracture: This is a special type of fracture sustained due to chronic repetitive injury (stress) causing a break in bony trabeculae.
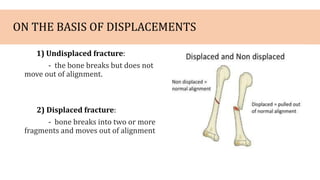
- 8. ON THE BASIS OF DISPLACEMENTS 1) Undisplaced fracture: - the bone breaks but does not move out of alignment. 2) Displaced fracture: - bone breaks into two or more fragments and moves out of alignment
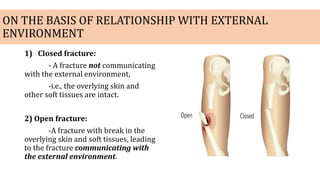
- 9. ON THE BASIS OF RELATIONSHIP WITH EXTERNAL ENVIRONMENT 1) Closed fracture: - A fracture not communicating with the external environment, -i.e., the overlying skin and other soft tissues are intact. 2) Open fracture: -A fracture with break in the overlying skin and soft tissues, leading to the fracture communicating with the external environment.
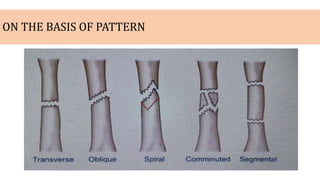
- 10. ON THE BASIS OF PATTERN
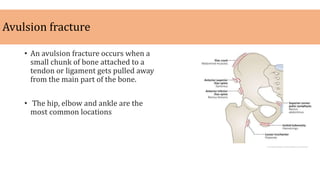
- 11. Avulsion fracture âĒ An avulsion fracture occurs when a small chunk of bone attached to a tendon or ligament gets pulled away from the main part of the bone. âĒ The hip, elbow and ankle are the most common locations
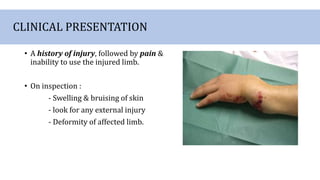
- 12. CLINICAL PRESENTATION âĒ A history of injury, followed by pain & inability to use the injured limb. âĒ On inspection : - Swelling & bruising of skin - look for any external injury - Deformity of affected limb.
- 13. âĒ On palpation of affected limb : - Raised temperature - Tenderness - Decreased range of movement - Abnormal mobility - Crepitus(a sound like produced by the grating of the ends of a fractured bone) - Signs of vascular & peripheral nerve injuries.
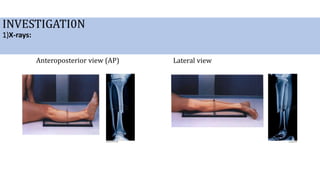
- 14. INVESTIGATI0N 1)X-rays: Anteroposterior view (AP) Lateral view
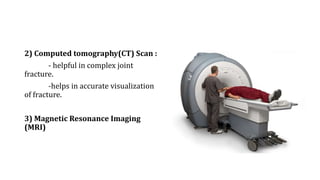
- 15. 2) Computed tomography(CT) Scan : - helpful in complex joint fracture. -helps in accurate visualization of fracture. 3) Magnetic Resonance Imaging (MRI)
- 16. TREATMENT Treatment of a fracture can be considered in three phases: âĒ Phase I - Emergency care âĒ Phase II - Definitive care âĒ Phase III - Rehabilitation
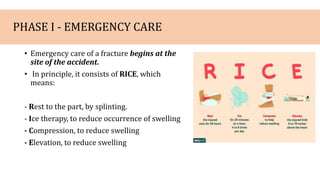
- 17. PHASE I - EMERGENCY CARE âĒ Emergency care of a fracture begins at the site of the accident. âĒ In principle, it consists of RICE, which means: - Rest to the part, by splinting. - Ice therapy, to reduce occurrence of swelling - Compression, to reduce swelling - Elevation, to reduce swelling
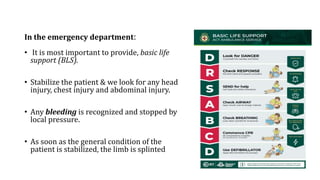
- 18. In the emergency department: âĒ It is most important to provide, basic life support (BLS). âĒ Stabilize the patient & we look for any head injury, chest injury and abdominal injury. âĒ Any bleeding is recognized and stopped by local pressure. âĒ As soon as the general condition of the patient is stabilized, the limb is splinted
- 19. PHASE II - DEFINITIVE CARE Fundamental principles of fracture treatment: (i) Reduction (ii) Immobilization ; and (iii) Preservation of functions.
- 20. i) Reduction âĒ Reduction is the technique of âsettingâ a displaced fracture to proper alignment. âĒ This may be done - non-operatively (closed) - operatively (open)
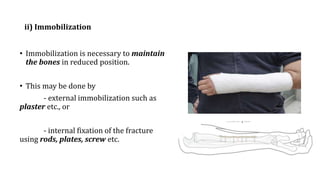
- 21. ii) Immobilization âĒ Immobilization is necessary to maintain the bones in reduced position. âĒ This may be done by - external immobilization such as plaster etc., or - internal fixation of the fracture using rods, plates, screw etc.
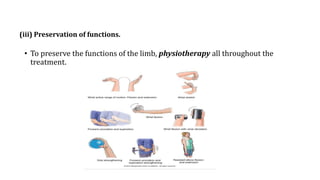
- 22. (iii) Preservation of functions. âĒ To preserve the functions of the limb, physiotherapy all throughout the treatment.
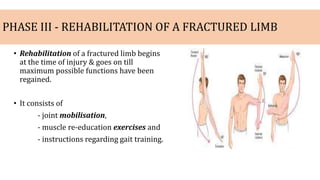
- 23. PHASE III - REHABILITATION OF A FRACTURED LIMB âĒ Rehabilitation of a fractured limb begins at the time of injury & goes on till maximum possible functions have been regained. âĒ It consists of - joint mobilisation, - muscle re-education exercises and - instructions regarding gait training.
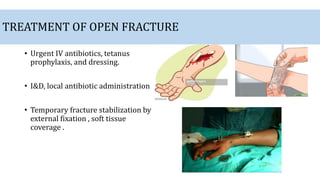
- 24. TREATMENT OF OPEN FRACTURE âĒ Urgent IV antibiotics, tetanus prophylaxis, and dressing. âĒ I&D, local antibiotic administration âĒ Temporary fracture stabilization by external fixation , soft tissue coverage .
- 25. COMPLICATION OF FRACTURE âĒ Complications of fractures can be classified into three broad groups depending upon their time of occurrence. âĒ These are as follows: a) Immediate complications â occurring at the time of the fracture. b) Early complications â occurring in the initial few days after the fracture. c) Late complications â occurring a long time after the fracture
- 26. Immediate complications 1) Hypovolemic shock - due to blood loss - treated with intravenous fluid & blood transfusion. 2) Injury to major vessels 3) Injury to muscles, tendons & joints.
- 27. Early complications 1) Fat embolism syndrome 2) DVT and Pulmonary embolism 3) Crush syndrome 4) Infection 5) Compartment syndrome
- 28. FAT EMBOLISM SYNDROME - Occlusion of small vessels by fat globules which is originate from fracture bone marrow. - Presenting features are in the form of two distinct types: (i) cerebral; and (ii) pulmonary - Treatment consists of - respiratory support, - heparinisation, - intravenous low molecular weight dextran and - corticosteroids.
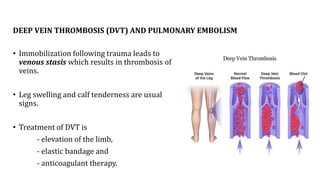
- 29. DEEP VEIN THROMBOSIS (DVT) AND PULMONARY EMBOLISM âĒ Immobilization following trauma leads to venous stasis which results in thrombosis of veins. âĒ Leg swelling and calf tenderness are usual signs. âĒ Treatment of DVT is - elevation of the limb, - elastic bandage and - anticoagulant therapy.
- 30. CRUSH SYNDROME âĒ This syndrome results from massive crushing of the muscles, commonly during earthquakes, air raids & mining. âĒ Crushing of muscles results in entry of myohaemoglobin into the circulation, leading to acute renal tubular necrosis. âĒ Stop bleeding by applying direct pressure. Cover the area with a wet cloth or bandage.
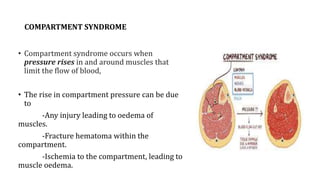
- 31. COMPARTMENT SYNDROME âĒ Compartment syndrome occurs when pressure rises in and around muscles that limit the flow of blood, âĒ The rise in compartment pressure can be due to -Any injury leading to oedema of muscles. -Fracture hematoma within the compartment. -Ischemia to the compartment, leading to muscle oedema.
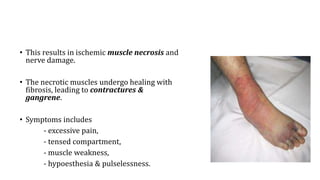
- 32. âĒ This results in ischemic muscle necrosis and nerve damage. âĒ The necrotic muscles undergo healing with fibrosis, leading to contractures & gangrene. âĒ Symptoms includes - excessive pain, - tensed compartment, - muscle weakness, - hypoesthesia & pulselessness.
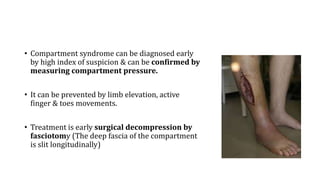
- 33. âĒ Compartment syndrome can be diagnosed early by high index of suspicion & can be confirmed by measuring compartment pressure. âĒ It can be prevented by limb elevation, active finger & toes movements. âĒ Treatment is early surgical decompression by fasciotomy (The deep fascia of the compartment is slit longitudinally)
- 34. Late complications 1) Malunion 2) Delayed union 3) Non-union 4) Avascular necrosis 5) Joint stiffness 6) Osteomyelitis 7) Osteoarthritis
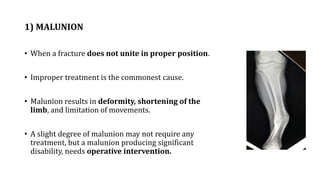
- 35. 1) MALUNION âĒ When a fracture does not unite in proper position. âĒ Improper treatment is the commonest cause. âĒ Malunion results in deformity, shortening of the limb, and limitation of movements. âĒ A slight degree of malunion may not require any treatment, but a malunion producing significant disability, needs operative intervention.
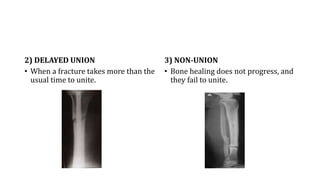
- 36. 2) DELAYED UNION âĒ When a fracture takes more than the usual time to unite. 3) NON-UNION âĒ Bone healing does not progress, and they fail to unite.
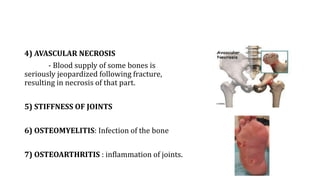
- 37. 4) AVASCULAR NECROSIS - Blood supply of some bones is seriously jeopardized following fracture, resulting in necrosis of that part. 5) STIFFNESS OF JOINTS 6) OSTEOMYELITIS: Infection of the bone 7) OSTEOARTHRITIS : inflammation of joints.
- 38. THANK YOU