



















Congenital vertical talus
- 1. Pediatric foot deformities Dr Alamzeb Khan MBBS,MCPS,MS(Orth),FCPS(Ortho) PROFESSOR DEPARTMENT OF ORTHOPAEDICS AYUB MEDICAL TEACHING INSTITUTION ABBOTTABAD
- 2. Why paediatric foot is different? • • Growing bones and soft tissues • Occult associated abnormalities • Training the soft tissues • Resultant secondary deformities • Pyschological and social impact
- 4. • Irreducible dorsal dislocation of the navicular on the talus producing a rigid flatfoot deformity present at birth
- 5. • CVT maybe associated with neuromuscular disorders such as AMC and myelomenningocele. • It can aslo occur as isolated congenital anomaly. • 50% bilateral • M:F ratio of 2:1
- 6. • Pathoanatomy Congenital vertical talus usually can be detected at birth by the presence of a rounded prominence of the medial and plantar surfaces of the foot produced by the abnormal location of the head of the talus.
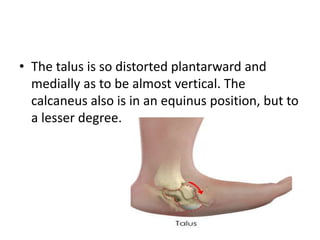
- 7. • The talus is so distorted plantarward and medially as to be almost vertical. The calcaneus also is in an equinus position, but to a lesser degree.
- 8. • As the foot develops and weight bearing is begun the talus becomes shaped like an hourglass but remains in so marked an equinus position that its longitudinal axis is almost the same as that of the tibia, and only the posterior third of its superior articular surface articulates with the tibia.
- 9. • The calcaneus remains in an equinus position also and becomes displaced posteriorly, and the anterior part of its plantar surface becomes rounded. • Callosities develop beneath the anterior end of the calcaneus and along the medial border of the foot superficial to the head of the talus. • When full weight is borne, the forefoot becomes severely abducted, and the heel does not touch the floor. Adaptive changes occur in the soft structures. All the capsules, ligaments, and tendons on the dorsum of the foot become contracted. The posterior tibial and peroneus longus and brevis tendons may come to lie anterior to the malleoli and act as dorsiflexors rather than plantar flexors.
- 10. • Radiographs Recommended views are AP, oblique and lateral foot Findings on lateral view • vertically positioned talus & dorsal dislocation of navicular line along long axis of talus passes below the first metatarsal- cuneiform axis before ossification of navicular at age 3, the first metatarsal is used as a proxy for the navicular on radiographic evaluation.
- 11. • AP • talocalcaneal angle > 40° (20-40° is normal)
- 12. • alternative views • forced plantar flexion lateral radiograph is diagnostic shows persistent dorsal dislocation of the talonavicular joint • oblique talus reduces on this view • Meary's angle > 20° (between line of longitudinal axis of talus and longitudinal axis of 1st metatarsal) • forced dorsiflexion lateral reveals fixed equinus
- 14. • MRI • neuraxial imaging should be performed to rule out neurologic disorder
- 15. • Differential Diagnosis • Oblique talus – reduces with forced plantar flexion – treatment is observation vs casting • Calcaneovalgus foot deformity • Posteromedial tibial bowing • Tarsal coalition • Paralytic pes valgus • Pes planovalgus
- 16. • Treatment • Nonoperative • serial manipulation and casting • indications • indicated preoperatively to stretch the dorsolateral soft-tissue structures • foot is manipulated into inversion and plantarflexion • typically still requires closed vs open pinning of the talonavicular joint with percutaneous achilles tenotomy
- 18. • Operative • surgical release and talonavicular reduction and pinning indications • indicated in most cases • performed at 6-12 months of age technique • involves pantalar release with concomitant lengthening of peroneals, Achilles, and toe extensors • talonavicular joint is reduced and pinned while reconstruction of the plantar calcaneonavicular (spring) ligament is performed • concomitant tibialis anterior transfer to talar neck.
- 20. • minimally invasive correction • indications new technique performed in some centers to avoid complications associated with extensive surgical releases. Technique • principles for casting are similar to the Ponseti technique used clubfoot
- 21. • serial casting utilized to stretch contracted dorsal and lateral soft tissue structures and gradually reduced talonavicular joint • once reduction is achieved with cast, closed or open reduction is performed and secured with pin fixation • percutaneous achilles tenotomy is required to correct the equinus deformity.
- 22. • talectomy – indicated in resistant case • triple arthrodesis – as salvage procedure for older children<12 years of age.
- 23. • Complications • Missed vertical talus • reconstructive options are less predictable after age 3, and patients may require triple arthrodesis as salvage procedure