










































Measles, Mumps, Rubella, Chicken pox
- 1. MMR & CHICKEN POX Dr. Gracy Paulin Assistant Professor Department of community medicine Government Thoothukudi Medical College
- 2. Outline ŌĆó Epidemiology triad ŌĆó Chicken pox ŌĆó Measles ŌĆó Mumps ŌĆó Rubella ŌĆó MR/MMR vaccines ŌĆó Small pox
- 4. CHICKEN POX
- 5. CHICKEN POX ŌĆó Also called as varicella ŌĆó Fever, malaise and rash ŌĆó Chicken pox and herpes zoster ŌĆó Case fatality rate is low
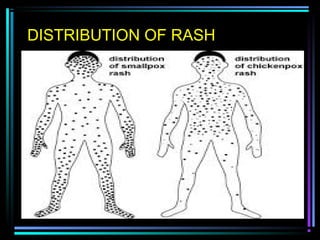
- 8. STAGES OF CHICKEN POX
- 9. CHARACTERISTICS OF RASH CrustingCrusting VesicleŌĆ£dew dropsŌĆØVesicleŌĆ£dew dropsŌĆØ PapulePapule
- 11. COMPLICATIONS OF CHICKEN POX ŌĆó Varicella haemorrhagica ŌĆó Pneumonia ŌĆó Encephalitis ŌĆó Acute cerebellar ataxia ŌĆó ReyeŌĆÖs syndrome ŌĆó Acute retinal necrosis ŌĆó Pitted scars ŌĆó Secondary bacterial infections ŌĆó Congenital varicella syndrome
- 12. LAB DIAGNOSIS & CONTROL ŌĆó Usually clinical ŌĆó Detecting viral DNA using PCR or through isolation ŌĆó Control: notification, isolation and disinfection ŌĆó Treatment: Acyclovir
- 13. IMMUNIZATION
- 14. MEASLES
- 15. MEASLES Measles is a leading cause of childhood deaths in developing countries Annually around 30 million cases of Measles are seen and about 9 lakh children die because of Measles Measles still kills about million people, annually
- 16. MEASLES (contd) Next disease amenable for eradication Challenges in elimination: Weak immunization system High infectious nature Inaccessible population Increasing refusal of immunization Changing epidemiology Gaps in human and financial resources
- 17. MEASLES IN INDIA ŌĆó Major cause of childhood mortality and morbidity ŌĆó 2% of under 5 mortality in India ŌĆó Most cases in tribal and remote areas go unreported ŌĆó Incidence is steadily declining
- 18. RNA paramyxovirus 6 months To 3 years Seasonal trend Measles
- 20. CHARACTERISTICS OF RASH Initial symptoms : high fever (103-105┬░F) & skin rash Followed by cough, runny nose, and/or conjunctivitis Rash usually appears about 14 days after exposure and lasts 5 - 6 days It begins at the hairline, then involves the face and upper neck Over next 3 days, rash gradually proceeds downward & outward, reaching hands & feet ŌĆō becomes confluent
- 21. KOPLIKŌĆÖS SPOTS
- 22. RASH IN MEASLES
- 24. 1. Respiratory ’ü« Otitis media, pneumonia, sec. bact. pneumonia ’ü« Laryngitis, croup, bronchitis 2. CNS ’ü« Encephalitis ŌĆō head ache, convulsions, coma ’ü« SSPE ŌĆō slow, months after, MR 3. Gastro-intestinal ’ü« Gastro-enteritis, Heapatitis, mescentric adenitis. Complications of Measles
- 25. CONTROL OF AN OUTBREAK ŌĆó Isolation of cases for 7 days after rash ŌĆó Immunization of contacts ŌĆó Immunization at the beginning of an epidemic
- 26. MUMPS
- 27. Mumps More than 85% of children become susceptible to mumps by the age of 9-12 months and continue to be so in the first 5 years of life It is estimated that about 8.5 - 9 lakh cases of mumps occur in our country every year.
- 28. Myxovirus parotiditis 5 to 9 years children Seasonal trend Mumps
- 29. Obvious sign of mumps is swelling of parotid region, because of Acute parotitis. Swelling usually lasts for 10 days with fever, Ear-ache, difficulty to talk, eat, open the mouth for 1-6 days. Affects various organs like salivary glands - Parotid glands, kidneys, testicles (Males), ovaries (females), pancreas, breast and joints┬Ā The symptoms- signs of Mumps
- 30. About 20% people who get mumps develop a painful swelling of testicles (Orchitis) and 50% will end up with testicular atrophy. Only 15% of cases of orchitis are bilateral in which case may leads to infertility. Mumps can also affect reproductive organs in females - oophoritis Sensori-neural (SN) deafness is a chronic compllication Mumps can also cause Asceptic Meningitis, joint pain, pancreatitis, myocarditis and mastitis Complications of Mumps
- 31. RUBELLA
- 33. RNA virus Togavirusfamily 3 to 10 years children Seasonal trend Rubella
- 34. Rubella - PNAR Sub-clinical, very mild viral illness, Dx. often missed Post auricular, sub occipital or cervical adenopathy Rash mainly face, never confluent, later extends ŌĆō body Fever may or may not occur, usually low grade, mild Complications ŌĆō rare ŌĆō arthritis, TCP, Haeg., Encephalt. Rubella in during pregnancy may lead to miscarriage.
- 37. The incidence of deformities in the various stages of pregnancy 3-11 weeks 100% infected fetus 12 weeks 80% infected fetus 13-14 weeks 54% infected fetus 15-16 weeks 35% infected fetus 23-26 weeks 25% infected fetus Time of maternal infection Result
- 38. The incidence of deformities in India Several studies have clearly shown the link between congenital defects and Rubella in Indian Children Study Defect Incidence due to Rubella Chennai Congenital deafness 29% Madurai Congenital cataract 26.3% Delhi Congenital malformations 21% (12000 samples)
- 39. The treatment for Rubella Unfortunately there is no treatment for Rubella. Vaccination is the only way to prevent all these complications In fact, 123 countries i.e. more than 57% of the countries include Rubella vaccine in their schedule Sri Lanka has already included the vaccine in their EPI program
- 40. Rubella vaccine should be given to All girls at puberty (9 years and above) All women of child bearing age and Hospital workers After vaccination at least of 3 months of contraception if missed, Post delivery to protect subsequent pregnancies
- 41. MR/MMR VACCINE
- 42. 1. To ensure adequate protection against Measles to all children, the WHO, American Academy of Paediatrics (AAP) and also the Indian Academy of Paediatrics (IAP) recommend use of two doses of Measles vaccine. 2. As perthe recommendation of the IAP, ŌĆó the first dose should be given at 9 months and ŌĆó the second dose should be given at 16 to 24 months Recommendations
- 43. Vaccine schedule Measles Vaccine at the age of 9 months MMR Vaccine at 12-15 months If missed any time up to 13 years of age
- 44. Small pox ŌĆó Last known case in India ŌĆō May 1975 ŌĆó Eradication ŌĆō April 1977 ŌĆó Government research centres in Russia and US ŌĆó Potential biological weapon
- 45. SUMMARY
- 46. THANK YOU
Editor's Notes
- #6: Herpes zoster ŌĆō occurs in aged individuals when cell mediated immunity declines due to reactivation of latent varicella virus. Severe in pregnant women, infants and immunocompromised individuals.
- #7: Mode of transmission ŌĆō contagious disease and through oropharyngeal secretions, droplet nuclei Life long immunity Secondary attack rate ŌĆō 90% Period of infectivity ŌĆō next slide. Host: children; life long immunity; pregnancy ŌĆō less than 20 weeks - congenital varicella syndrome; Environment: winter, spring, coolest, driest months. Heat labile.
- #11: Centrifugal in distribution; absent in palms and soles; may involve axilla, buccal mucosa
- #12: ReyeŌĆÖs syndrome: acute encephalopathy with fatty degeneration of liver Cogenital varicella syndrome: foetal wastage, cutaneous scars, atrophied limbs, microcephaly, chorioretinitis, deafness, cerebro-cortical atrophy
- #14: Age: 12 to 18 months VZIG: given within 72 hours of exposure; intramuscular route;
- #19: Mode of transmission ŌĆō contagious disease and through oropharyngeal secretions, droplet nuclei Life long immunity Secondary attack rate ŌĆō 90% Period of infectivity ŌĆō next slide. Host: children; life long immunity; malnourished children Environment: winter, spring, coolest, driest months. Overcrowding
- #28: Although the morbidity of mumps is high, the mortality due to this disease is negligible.
- #29: Subclinical infections occur. Mode of transmission ŌĆō contagious disease and through oropharyngeal secretions, droplet nuclei Life long immunity Secondary attack rate ŌĆō 90% Period of infectivity ŌĆō next slide. Host: children; life long immunity; malnourished children; Pregnancy ŌĆō spontaneous abortion in 25% cases Environment: winter, spring, coolest, driest months. Overcrowding
- #34: Subclinical infections occur. Major difference between measles and rubella. Mode of transmission ŌĆō contagious disease and through oropharyngeal secretions, droplet nuclei Life long immunity Secondary attack rate is low Host: children; life long immunity; Pregnancy ŌĆō 40% are susceptible Environment: winter, spring, coolest, driest months. Overcrowding
- #45: Caused by variola virus. Characterized by sudden onset of fever, headache, backache, vomiting and convulsions. Rash ŌĆō 3rd day of fever. By eradicating small pox, we have prevented 2 million deaths per year. Despite the eradication of small pox, surveillance is still going on. WHO reserves a stock of vaccine sufficient for 200 million people, if an emergency arises.