Acute appendicitis
•Download as PPTX, PDF•
9 likes•442 views

Appendicitis is inflammation of the appendix that requires emergency treatment. It is commonly caused by obstruction of the appendix lumen, usually by lymphoid hyperplasia. Clinical features include abdominal pain shifting to the right lower quadrant, nausea, vomiting, and fever. Diagnosis involves blood tests, ultrasound or CT scan. Treatment is surgical removal of the inflamed appendix, which can be done through traditional open surgery or laparoscopically. Complications can include perforation leading to peritonitis if not treated promptly.















Acute appendicitis
- 2. 1 STARTING WITH DEFINITION ?? 2 SURGICAL ANATOMY 3 ETIOLOGY AND PATHOPHYSIOLOGY 4 TYPES 5 CLINICAL FEATURES 6 OUTCOME 7 DIFFERENTIAL DIAGNOSIS 8 SCORING SYSTEM 9 INVESTIGATIONS 10 MANAGEMENT PLAN 11 COMPLICATIONS 12 VIDIO DEMONSTRATION
- 3. Appendicitis is inflammation of the appendix and is a medical emergency. Many cases of appendicitis require removal of the inflamed appendix due to the high mortality associated with rupture of the appendix, which may lead to severe complications such as peritonitis and sepsis. Appendicitis was first described by Reginald Fitz in 1886 and is today recognized as one of the most common and significant causes of severe acute abdominal pain worldwide.
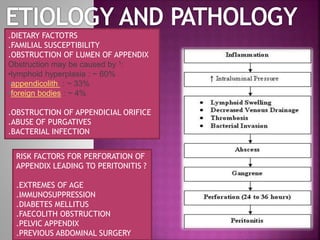
- 5. .DIETARY FACTOTRS .FAMILIAL SUSCEPTIBILITY .OBSTRUCTION OF LUMEN OF APPENDIX Obstruction may be caused by 1: •lymphoid hyperplasia : ~ 60% •appendicolith : ~ 33% •foreign bodies : ~ 4% .OBSTRUCTION OF APPENDICIAL ORIFICE .ABUSE OF PURGATIVES .BACTERIAL INFECTION RISK FACTORS FOR PERFORATION OF APPENDIX LEADING TO PERITONITIS ? .EXTREMES OF AGE .IMMUNOSUPPRESSION .DIABETES MELLITUS .FAECOLITH OBSTRUCTION .PELVIC APPENDIX .PREVIOUS ABDOMINAL SURGERY
- 6. 1 ACUTE CATARRHAL ( NON OBSTRUCTIVE ) APPENDICITIS 2 OBSTRUCTIVE ACUTE APPENDICITS
- 7. SYMPTOMS . ABDOMINAL PAIN WHICH SHIFTS . ANOREXIA . NAUSEA AND VOMITING . FEVER . GASTRIC FUNCTION UPSET ( DIARRHEA AND CONSTIPATION)
- 8. .LOCALIZED TENDERNESS IN RIF .MUSCLE GUARDING AND RIGIDITY .POINTING SIGN .COUGH/DUNPHY’S SIGN .REBOUND TENDERNESS .ROVSING’S SIGN .PSOAS SIGN .OBTURATOR SIGN
- 9. .RESOLUTION .ULCERATION .SUPPURATION .FIBROSIS .GANGRENE .PHLEGMONOUS MASS .APPENDICULAR ABCESS .MUCOCOELE OF APPENDIX .GENERAL PERITONITIS Mainly composed of greater omentum, edematous caecal wall, edematous portion of small intestine, perforated or otherwise inflamed appendix
- 12. Tzanakis Scoring Tzanakis and colleagues, in 2005 published a simplified system, now called the Tzanakis scoring system for appendicitis, to aid the diagnosis of appendicitis. It incorporates the presence 4 variables made up of specific signs and symptoms. .presence of right lower abdominal tenderness = 4 points and rebound tenderness = 3 points .laboratory findings: presence of white blood cells greater than 12,000 in the blood = 2 points .ultrasound finding: presence of positive ultrasound scan findings of appendicitis = 6 points A total score of 15 is the maximum that can be scored. Where a patient scores 8 or more points, there is greater than 96 percent chance that appendicitis exists..
- 13. 1: ROUTINE FULL BLOOD COUNT URINANALYSIS 2: SELECTIVE PREGNANCY TEST UREA AND ELECTROLYTES SUPINE ABDOMINAL RADIOGRAPH ULTRASOUND ABDOMEN/PELVIS CONTRAST ENHANCED CT SCAN ABDOMEN
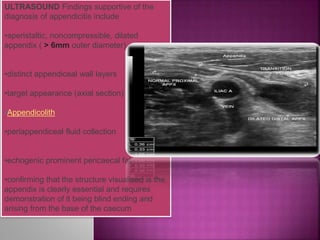
- 14. ULTRASOUND Findings supportive of the diagnosis of appendicitis include •aperistaltic, noncompressible, dilated appendix ( > 6mm outer diameter) •distinct appendiceal wall layers •target appearance (axial section) •Appendicolith •periappendiceal fluid collection •echogenic prominent pericaecal fat •confirming that the structure visualised is the appendix is clearly essential and requires demonstration of it being blind ending and arising from the base of the caecum
- 15. KEEP NPO START IV FLUIDS GIVE ANALGESIA FOR SEVER PAIN ROLE OF ANTIBIOTICS PLAN SURGERY CONVENTIONAL APPENDICECTOMY LAPROSCOPIC APPENDICECTOMY
- 16. BASIC STEPS .G/A GIVEN .ABDOMEN PREPARED AND DRAPED INCISION GIVEN OVER McBurney’s point ( GRID IRON INCISION) .VARIOUS LAYERS OF ABDOMINAL WALL OPENED .MUSCLES SPLIT ALONG LINE OF ITS FIBERS .ON ENTERING PERITONEUM APPENDIX IDENTIFIED ..MOBILIZED THEN LIGATED AND DIVIDED AT ITS BASE .LAYERS OF ABDOMINAL WALL THEN CLOSED IN TURN SKIN CLOSSED AND DRESSING DONE
- 17. Over the past decade, the outcomes of laparoscopic appendectomies have compared favorably to those for open appendectomies because of decreased pain, fewer postoperative complications, shorter hospitalization, earlier mobilization, earlier return to work, and better cosmesis. However, despite these advantages, efforts are still being made to decrease abdominal incision and visible scars after laparoscopy
- 18. EARLY LATE