Iapt stepped care
âĒDownload as PPT, PDFâĒ
2 likesâĒ2,164 views

The IAPT (Increasing Access to Psychological Therapies) programme aims to implement NICE-recommended psychological therapies for anxiety and depression on a national scale in England. It uses a stepped care model to provide the least intrusive but most effective treatment first. Services offer a range of evidence-based interventions including CBT, guided self-help, groups, computer-assisted therapy, and more intensive treatments. Challenges for the future include further integration with primary care, links to long-term conditions and employment support, and ensuring coherent services across commissioning bodies in the changing NHS landscape.











Iapt stepped care
- 1. STEPPED CARE MODEL Matt Broadway-Horner Programme lecturer in the mental health and social sciences faculty
- 3. Agenda âĒAims âĒWhat is IAPT? âĒThe Programme in London âĒChallenges, Opportunities and Discussion
- 4. Aims âĒGreater understanding of the IAPT programme and what it is trying to achieve âĒHow the programme has been rolled out, specific challenges for London and further work to be done by 2014 âĒWhere IAPT might sit in the new commissioning landscape âĒHow IAPT can fit in to wider primary care strategies including further engagement with primary care âĒWhat IAPT can offer local authorities and Health and
- 5. What is IAPT? âĒNational programme - implement NICE recommended psychological therapies for anxiety and depression. âĒFirst phase (2008-2010) - ÂĢ400,000,000 to train 3600 new therapists to treat a total of 900,000 people âĒSecond phase (2011-2014) - ÂĢ400,000,000 to train 2400 new therapists, treating 1,000,000 people a year(15% need). âĒOutcome monitoring - sessional measures - key indicators access, recovery, moving off sick pay/ benefits âĒPopulation approach - assessing need and developing services and a workforce with the relevant competencies to meet that need. âĒIncrease capacity - specific curricula developed for extensive training programme to train a new workforce - LI and HI staff âĒA âfullâ service consists of around 40 clinicians for a population of 250,000.
- 6. âIt was the practical work that made me realise I can do the things I feared and without doing them with the therapist I don't think Iâd have made nearly as much progressâ
- 7. The IAPT Argument (Depression Report 2006) âĒ Mental Health service provision often focuses on psychosis which deserves attention but affects 1% of population at any one time. âĒ Many more people suffer from anxiety and depression (approx.15% at any one time - 6 million people in England). âĒ Economic cost is huge (lost output ÂĢ17 billion pa, of which ÂĢ9 billion is a direct cost to the Exchequer). âĒ Effective psychological treatments exist. NICE Guidance recommends CBT for depression and all anxiety disorders plus some other treatments for individual conditions (EMDR for PTSD, Interpersonal Psychotherapy, Couples therapy, Counseling & Brief Dynamic Therapy for some levels of depression). âĒ Less than 5% of people with anxiety disorders or depression receive an evidence based psychological treatment. Patients show a 2:1 preference for psychological therapies versus medication âĒ Increased provision largely payâs for itself
- 8. Key Features of IAPT services âĒStepped care - least intrusive, most effective treatment is offered first âĒRange of evidence-based interventions âĒEasy access - self referrals âĒTarget under-represented groups âmulti lingual, older people âĒLinks to employment support âĒIntegrated with primary care âĒIntegration with other parts of mental health system
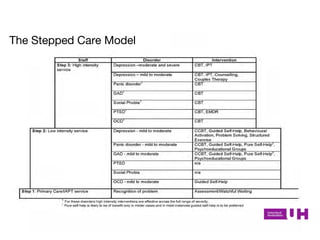
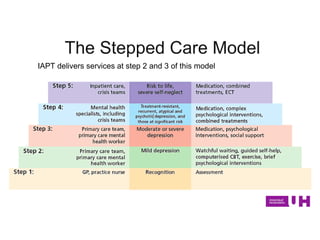
- 9. The Stepped Care Model
- 10. IAPT delivers services at step 2 and 3 of this model The Stepped Care Model
- 11. The IAPT Programme in London The IAPT programme in London has been one of graduated rollout and focussed on areas of highest deprivation first - this means that most of inner London has good coverage - outer London generally has less capacity and is less well resourced. Despite having an IAPT service in every PCT only about 60% geographical/population coverage.
- 12. The IAPT Programme in London âĒServices vary hugely in size with a large number unable to meet the needs of the local populations due to limited capacity and investment. The ability to meet need ranges from 0.23% to 11.42% and London as a whole is meeting 6.5% need. âĒLondon currently has a workforce of around 1000 psychological therapists with well over half of these being trained and funded directly by the programme. The majority of this workforce is concentrated in central London.
- 13. Challenges and Opportunities âĒDeveloping role in LTCs âĒIncreased risk of MH problems / impact on physical health outcomes âĒLink to developing LTC pathways âĒTraining for staff - balance between specialist skills and generic skills âĒDeveloping work with primary care teams âĒMUS â joint management âĒCollaborative care models â depression and LTCs/ MUS âĒBalance between close working with PC and efficient, centralised models âĒBalance between GP preference for more inclusive service and maximising recovery rates. âĒDeveloping public health approach âĒPrevention/ mental health promotion âĒTargeting specific groups to improve access âĒLinks with physical health programmes âĒLinks with social care/LAs âĒImpact of welfare reforms âĒEmployment â best way of providing this support âĒChildrenâs centres/ housing
- 14. Challenges and Opportunities âĒMake it local - integration with existing mental services âĒEnsuring coherent services with multiple providers âĒWho will be key players in decisions about commissioning IAPT services? âĒCCGs âĒHWBs âĒPublic Health âĒCommissioning Board
- 15. âĒ Activity scheduling â Increasing pleasure and achievement âĒ Thought challenging â Identifying and challenging negative automatic thoughts âĒ Problem solving â Exploring and breaking down problems into manageable tasks âĒ Via 1:1, telephone, groups and computer âĒ Computer Aided CBT â Beating the Blues â Fear Fighter CBT Interventions at Step 2
- 16. âĒ Based on modified CBT framework âĒ Same principles as many of the self-help books but support and encouragement of trained worker âĒ Oxford Cognitive Therapy Centre Self help manuals âĒ Maximum of 6 sessions, each 40-50mins âĒ Delivered in community settings; GP surgeries, libraries and Children Centres Step 2 Guided Self Help
- 17. âĒ Step 2 â Depression and Anxiety group â Introduction to CBT Skills â Turkish Access â Assertiveness â Stress group â Turkish stress group â Post Natal Adjustment â Employment â Fear Fighter Group âĒ Step 3 â Mindfulness CBT group â Social Anxiety group â Worry group â Trauma Recovery â Trauma Recovery Turkish Speaking Groups
- 18. You can find further information about the IAPT programme at: www.iapt.nhs.uk