




06-cardiac_muscle (2).pdf
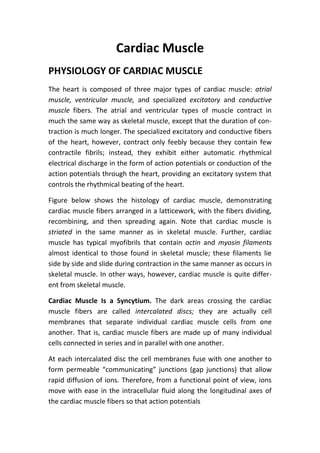
- 1. Cardiac Muscle PHYSIOLOGY OF CARDIAC MUSCLE The heart is composed of three major types of cardiac muscle: atrial muscle, ventricular muscle, and specialized excitatory and conductive muscle fibers. The atrial and ventricular types of muscle contract in much the same way as skeletal muscle, except that the duration of con- traction is much longer. The specialized excitatory and conductive fibers of the heart, however, contract only feebly because they contain few contractile fibrils; instead, they exhibit either automatic rhythmical electrical discharge in the form of action potentials or conduction of the action potentials through the heart, providing an excitatory system that controls the rhythmical beating of the heart. Figure below shows the histology of cardiac muscle, demonstrating cardiac muscle fibers arranged in a latticework, with the fibers dividing, recombining, and then spreading again. Note that cardiac muscle is striated in the same manner as in skeletal muscle. Further, cardiac muscle has typical myofibrils that contain actin and myosin filaments almost identical to those found in skeletal muscle; these filaments lie side by side and slide during contraction in the same manner as occurs in skeletal muscle. In other ways, however, cardiac muscle is quite differ- ent from skeletal muscle. Cardiac Muscle Is a Syncytium. The dark areas crossing the cardiac muscle fibers are called intercalated discs; they are actually cell membranes that separate individual cardiac muscle cells from one another. That is, cardiac muscle fibers are made up of many individual cells connected in series and in parallel with one another. At each intercalated disc the cell membranes fuse with one another to form permeable âcommunicatingâ junctions (gap junctions) that allow rapid diffusion of ions. Therefore, from a functional point of view, ions move with ease in the intracellular fluid along the longitudinal axes of the cardiac muscle fibers so that action potentials
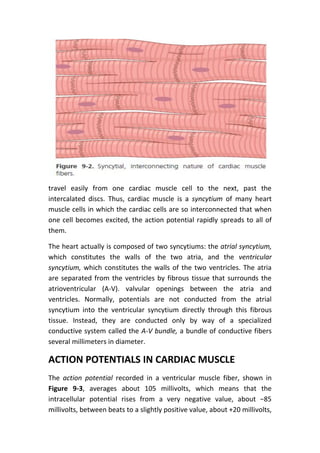
- 2. travel easily from one cardiac muscle cell to the next, past the intercalated discs. Thus, cardiac muscle is a syncytium of many heart muscle cells in which the cardiac cells are so interconnected that when one cell becomes excited, the action potential rapidly spreads to all of them. The heart actually is composed of two syncytiums: the atrial syncytium, which constitutes the walls of the two atria, and the ventricular syncytium, which constitutes the walls of the two ventricles. The atria are separated from the ventricles by fibrous tissue that surrounds the atrioventricular (A-V). valvular openings between the atria and ventricles. Normally, potentials are not conducted from the atrial syncytium into the ventricular syncytium directly through this fibrous tissue. Instead, they are conducted only by way of a specialized conductive system called the A-V bundle, a bundle of conductive fibers several millimeters in diameter. ACTION POTENTIALS IN CARDIAC MUSCLE The action potential recorded in a ventricular muscle fiber, shown in Figure 9-3, averages about 105 millivolts, which means that the intracellular potential rises from a very negative value, about â85 millivolts, between beats to a slightly positive value, about +20 millivolts,
- 3. during each beat. After the initial spike, the membrane remains depolarized for about 0.2 second, exhibiting a plateau, followed at the end of the plateau by abrupt repolarization. The presence of this plateau in the action potential causes ventricular contraction to last as much as 15 times as long in cardiac muscle as in skeletal muscle. At least two major differences between the membrane properties of cardiac and skeletal muscle account for the prolonged action potential and the plateau in cardiac muscle. First, the action potential of skeletal muscle is caused almost entirely by the sudden opening of large numbers of fast sodium channels that allow tremendous numbers of sodium ions to enter the skeletal muscle fiber from the extracellular fluid. These channels are called âfastâ channels because they remain open for only a few thousandths of a second and then abruptly close. At the end of this closure, repolarization occurs, and the action potential is over within another thousandth of a second or so. In cardiac muscle, the action potential is caused by opening of two types of channels: (1) the same voltage-activated fast sodium channels as those in skeletal muscle and (2) another entirely different population of L-type calcium channels (slow calcium channels), which are also called calcium-sodium channels. This second population of channels differs
- 4. from the fast sodium channels in that they are slower to open and, even more important, remain open for several tenths of a second. During this time, a large quantity of both calcium and sodium ions flows through these channels to the interior of the cardiac muscle fiber, and this activity maintains a prolonged period of depolarization, causing the plateau in the action potential. Further, the calcium ions that enter during this plateau phase activate the muscle contractile process, whereas the calcium ions that cause skeletal muscle contraction are derived from the intracellular sarcoplasmic reticulum. The second major functional difference between cardiac muscle and skeletal muscle that helps account for both the prolonged action potential and its plateau is this: Immediately after the onset of the action potential, the permeability of the cardiac muscle membrane for potassium ions decreases about fivefold, an effect that does not occur in skeletal muscle. the decreased potassium permeability greatly decreases the outflux of positively charged potassium ions during the action potential plateau and thereby prevents early return of the action potential voltage to its resting level. Summary of Phases of Cardiac Muscle Action Potential Figure below summarizes the phases of the action potential in cardiac muscle and the ion flows that occur during each phase. Phase 0 (depolarization), fast sodium channels open. When the cardiac cell is stimulated and depolarizes, the membrane potential becomes more positive. Voltage-gated sodium channels (fast sodium channels) open and permit sodium to rapidly flow into the cell and depolarize it. The membrane potential reaches about +20 millivolts before the sodium channels close. Phase 1 (initial repolarization), fast sodium channels close. The sodium channels close, the cell begins to repolarize, and potassium ions leave the cell through open potassium channels. Phase 2 (plateau), calcium channels open and fast potassium channels close. A brief initial repolarization occurs and the action potential then
- 5. plateaus as a result of (1) increased calcium ion permeability and (2) decreased potassium ion permeability. Phase 3 (rapid repolarization), calcium channels close and slow potassium channels open. The closure of calcium ion channels and increased potassium ion permeability, permitting potassium ions to rapidly exit the cell, ends the plateau and returns the cell membrane potential to its resting level. Phase 4 (resting membrane potential) averages about â90 millivolts. EXCITATION-CONTRACTION COUPLINGâ FUNCTION OF CALCIUM IONS AND THE TRANSVERSE TUBULES The term âexcitation-contraction couplingâ refers to the mechanism by which the action potential causes the myofibrils of muscle to contract. As is true for skeletal muscle, when an action potential passes over the cardiac muscle membrane, the action potential spreads to the interior of the cardiac muscle fiber along the membranes of the transverse (T) tubules. The T tubule action potentials cause release of calcium ions into the muscle sarcoplasm from the sarcoplasmic reticulum. In another few thousandths of a second, these calcium ions diffuse into the myofibrils
- 6. and catalyze the chemical reactions that promote sliding of the actin and myosin filaments along one another, which produces the muscle contraction. Thus far, this mechanism of excitation-contraction coupling is the same as that for skeletal muscle, but there is a second effect that is quite different. In addition to the calcium ions that are released into the sarcoplasm , calcium ions also diffuse into the sarcoplasm from the T tubules themselves at the time of the action potential, which opens voltage-dependent calcium channels in the membrane of the T tubule (Figure 9-6). Calcium entering the cell then activates calcium release channels in the sarcoplasmic reticulum membrane, triggering the release of calcium into the sarcoplasm. Without the calcium from the T tubules, the strength of cardiac muscle contraction would be reduced considerably because the sarcoplasmic reticulum of cardiac muscle is less well developed than that of skeletal muscle and does not store enough calcium . At the end of the plateau of the cardiac action potential, the influx of calcium ions to the interior of the muscle fiber is suddenly cut off, and calcium ions in the sarcoplasm are rapidly pumped back out of the muscle fibers into both the sarcoplasmic reticulum and the T tubuleâ extracellular fluid space. (see Figure 9-6). Calcium ions are also removed from the cell by a sodium-calcium exchanger. The sodium that enters the cell during this exchange is then transported out of the cell by the sodium-potassium ATPase pump. As a result, the contraction ceases until a new action potential comes along.