Igene - PhD SICSA Poster Presentation
ŌĆó
1 likeŌĆó196 views

The document compares four accident analysis models - Events and Causal Factors (ECF), Human Factors Analysis and Classification System (HFACS), System-Theoretic Accident Model and Processes (STAMP), and Rasmussen's AcciMaps - in their analysis of a medication dosing error case study involving a computerized physician order entry (CPOE) system. It finds that while the models identify common causes, such as human-computer interaction issues, AcciMaps and STAMP provide the deepest analysis by examining contributing factors across multiple levels of the sociotechnical system, but that the reliability of AcciMap analysis needs improvement for healthcare applications.
Igene - PhD SICSA Poster Presentation
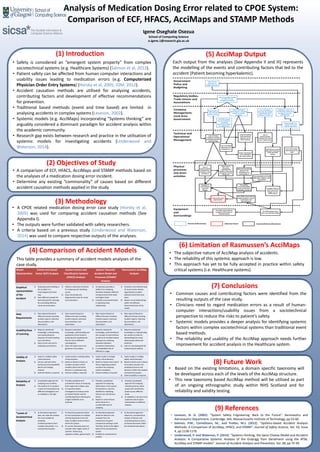
- 1. (4) Comparison of Accident Models This table provides a summary of accident models analyses of the case study. Analysis of Medication Dosing Error related to CPOE System: Comparison of ECF, HFACS, AcciMaps and STAMP Methods (1) Introduction ŌĆó Safety is considered an ŌĆ£emergent system propertyŌĆØ from complex sociotechnical systems (e.g. Healthcare Systems) (Salmon et al, 2012). ŌĆó Patient safety can be affected from human computer interactions and usability issues leading to medication errors (e.g. Computerized Physician Order Entry Systems) (Horsky et al, 2005; IOM, 2012). ŌĆó Accident causation methods are utilised for analysing accidents, contributing factors and development of effective recommendations for prevention. ŌĆó Traditional based methods (event and time based) are limited in analysing accidents in complex systems (Leveson, 2002). ŌĆó Systemic models (e.g. AcciMaps) incorporating ŌĆ£Systems thinkingŌĆØ are arguably considered a dominant paradigm for accident analysis within the academic community. ŌĆó Research gap exists between research and practice in the utilisation of systemic models for investigating accidents (Underwood and Waterson, 2014). (3) Methodology ŌĆó A CPOE related medication dosing error case study (Horsky et al, 2005) was used for comparing accident causation methods (See Appendix I). ŌĆó The outputs were further validated with safety researchers. ŌĆó A criteria based on a previous study (Underwood and Waterson, 2014) was used to compare respective outputs of the analyses. (6) Limitation of RasmussenŌĆÖs AcciMaps ŌĆó The subjective nature of AcciMap analysis of accidents. ŌĆó The reliability of this systemic approach is low. ŌĆó This approach has yet to be fully accepted in practice within safety critical systems (i.e. Healthcare systems). (8) Future Work ŌĆó Based on the existing limitations, a domain specific taxonomy will be developed across each of the levels of the AcciMap structure. ŌĆó This new taxonomy based AcciMap method will be utilised as part of an ongoing ethnographic study within NHS Scotland and for reliability and validity testing. (7) Conclusions ŌĆó Common causes and contributing factors were identified from the resulting outputs of the case study. ŌĆó Clinicians need to regard medication errors as a result of human- computer interactions/usability issues from a sociotechnical perspective to reduce the risks to patientŌĆÖs safety. ŌĆó Systemic models provides a deeper analysis for identifying systemic factors within complex sociotechnical systems than traditional event based methods. ŌĆó The reliability and usability of the AcciMap approach needs further improvement for accident analysis in the Healthcare system. Igene Oseghale Osezua School of Computing Science o.igene.1@research.gla.ac.uk (9) References ŌĆó Leveson, N. G. (2002). ŌĆ£System Safety Engineering: Back to the FutureŌĆØ. Aeronautics and Astronautics Department. Cambridge, MA, Massachusetts Institute of Technology, pp 53-60. ŌĆó Salmon, P.M., Cornelissen, M., and Trotter, M.J. (2012). ŌĆ£Systems-based Accident Analysis Methods: A Comparison of AcciMap, HFACS, and STAMPŌĆØ. Journal of Safety Science, Vol. 50, Issue 4, pp 1158-1170. ŌĆó Underwood, P. and Waterson, P. (2014). ŌĆ£Systems thinking, the Swiss Cheese Model and Accident Analysis: A Comparative Systemic Analysis of the Grayrigg Train Derailment using the ATSB, AcciMap and STAMP modelsŌĆØ. Journal of Accident Analysis and Prevention, Vol. 68, pp 75-94. (2) Objectives of Study ŌĆó A comparison of ECF, HFACS, AcciMaps and STAMP methods based on the analyses of a medication dosing error incident. ŌĆó Determine any existing ŌĆ£commonalityŌĆØ of causes based on different accident causation methods applied in the study. (5) AcciMap Output Each output from the analyses (See Appendix II and III) represents the modelling of the events and contributing factors that led to the accident (Patient becoming hyperkalemic). Model Characteristics Events and Causal Factor (ECF) Analysis Human Factors and Classification Systems (HFACS) Analysis System Theoretic Accident Model and Processes (STAMP) Analysis RasmussenŌĆÖs AcciMap Analysis Graphical representation of the Accident 1) Analysing events leading to the accident in a chronological and linear way. 2) Uses different symbols for denoting specific meanings thus providing effective visual communication. 1) Utilizes a taxonomy of failures for analysing and classifying causes. 2) Does not provide any diagrammatic tools for visual communication. 1) Its taxonomy provides a platform for analysing deviations between different components for both lower and higher levels. 2) Complex visual presentation in depicting these relationships. 1) Provides a very effective way of visual communication regarding the accident (adverse event) that took place 2) Depicts causal relationships within the different hierarchical levels of the model. Data Requirements 1) Data required based on different formats including incident reports, interview documentation, and observation. 1) Data required based on different formats including incident reports, interview documentation, and observation. 1) Data required based on different formats including incident reports, interview documentation, and observation. 1) Data required based on different formats including incident reports, interview documentation, and observation. Usability/Ease of Learning 1) Requires substantial knowledge, understanding and representing the sequence of events leading up to the failure. 2) Easy to learn and use for analysing causal factors. 1) Requires substantial knowledge, understanding and application of the model in analysing and classifying the failures into its different subcategories. 2) Does not require too much guidance in its analysis. 1) Requires substantial knowledge, understanding of the concept of control theory as well as its resultant system taxonomy for analysing deviations between component interactions. 2) A considerable level of difficulty in usage. 1) Requires substantial knowledge in understanding but simple to utilize for representing the causal relationships (distal and proximal). 2) Lack of a standard guide for conducting the analysis. Validity of Analysis 1) Useful in multiple safety critical domains. 2) Can be used with other techniques including MORT, Barrier and Change Analysis. 3) External validity is required. 1) Useful model in multiple safety critical domains. 2) Based on ReasonŌĆÖs theory of accident causation which classifies latent and active failures in a systematic way. 3) External validity is required. 1) Useful model in multiple safety critical domains. 2) Based on System and Control theory regarding accident causation for analysing system complexity. 3) External validity is required. 1) Useful model in multiple safety critical domains. 2) Based on RasmussenŌĆÖs theory of accident causation for analysing structure and dynamics within the complex sociotechnical system. 3) External validity is required. Reliability of Analysis 1) A qualitative approach for analysing case incidents. 2) The analysis of an accident is open to interpretation by different investigators and so reliability is not high. 1) Provides qualitative and quantitative means of analysing both single and multiple cases. 2) Its taxonomy allows investigators to analyse active and latent failures and the contributing factors allowing for a higher reliability to be achieved. 1) Provides a qualitative approach for analysing dysfunctions in the system. Its taxonomy is not very detailed for classifying failures and contributory factors. 2) Based on control theory which allows for a considerable level of reliability. 1) Provides a qualitative approach for analysing multiple proximal, distal causes and contributory factors across different levels. 2) Its reliability is low due to its subjective nature (open interpretation to different analysts). *Levels of Sociotechnical Analysis 1) Its theoretical approach does not make the method the most suitable for analysing incidents/accidents from complex interactions in a sociotechnical system. 1) Its theoretical approach allows for the classification of multiple contributing factors from the lower to higher levels of failure within the system. 2) Its current taxonomy does not consider other higher levels of systemic failures (e.g. regulatory bodies, government) 1) Its theoretical approach allows for failures to be analysed from the interactions of system components existing in both the lower levels to the higher levels of the sociotechnical system. 2) Suitable for sociotechnical analysis. 1) Its theoretical approach allows for a sociotechnical analysis of failures and contributing factors across all hierarchical levels within the sociotechnical system. Government Policy and Budgeting Company Management, Local Area Government Regulatory bodies, Trade Unions and Associations Technical and Operational Management Physical processes and Actor activities Equipment and Surroundings The CPOE system had a poor user interface design Lack of clinical handover training and implementation plan/strategy Provider B administered more KCI dosage There was no discussion regarding the patientŌĆÖs KCI levels during the clinical changeover Miscommunication between the attending nurse and Provider A Lack of communication between the Provider A and Provider B Inadequate resources for planning, hiring and training of new and existing staff OrganizationŌĆÖs Low risk and safety culture Lack of proactive approaches in analysing health-IT related incidents Government priorities on budget allocation Staff did not receive adequate training in using the CPOE system Lack of oversight relating to safety and risk management policies Limited budget for IT maintenance and optimal operations Patient becomes Hyperkalemic Events (Inferences) Adverse Event The CPOE system did not recognize instructions in comment boxes Under reporting of errors relating to the CPOE system Lack of communication between the users and IT department Lack of feedback between the health organization and Software Vendors Lack of Incident reporting on IT related errors The attending nurse had difficulties reading in the instructions The CPOE screen did not display patient's recent result before KCI administration Underestimating risks associated with the use of CPOE systems The patient received multiple doses of KCI than originally intended Provider A did not enter the correct dosage into the CPOE system Poor information flow between the staff The CPOE system was not tested in a simulated environment before live deployment Events/Actions/Decisions