





















Pediatric burns
- 1. Presented by :Mrs Rupal Patel . Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 2. âĒ Burns and scalds account for 6% of peadiatric injuries. âĒ The majority involve pre-school children,burns being most common between 1-2 yrs,flame burns bet 5-18 yrs. âĒ House fires are the cause of most fatal burns with smoke inhalation being the immediate cause of death in many cases. âĒ Scalds are most commonly associated with hot drinks in toddlers, also occur with over heated bath water and hot cooking oil. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 3. Severity of burn is related with 1.Temperature and 2.Duration of contact.e.g., âĒ At 44c - tissue damage occurs with 6hrs of contact with heat source âĒ While At 70c epidermal injury occurs in just 1sec. Mrs.Rupal Patel, Assistant Professor, Sumandeep Nursing College
- 4. Wounds caused by exposure to: 1. Excessive heat 2. Chemicals 3. Fire/steam 4. Radiation 5. Electricity 4 5Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 5. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 6. Wound excision until fine punctate bleeding occurs Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 7. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 8. s Partial thickness burn = involves epidermis Deep partial thicknes =involves dermis Full thickness = involves all of skin Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 9. Involves only the epidermis âĒ Tissue will blanch with pressure âĒ Tissue is erythematous and often painful âĒ Involves minimal tissue damage âĒ Sunburn Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
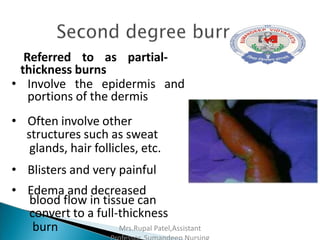
- 10. Referred to as partial- thickness burns âĒ Involve the epidermis and portions of the dermis âĒ Often involve other structures such as sweat glands, hair follicles, etc. âĒ Blisters and very painful âĒ Edema and decreased blood flow in tissue can convert to a full-thickness burn Mrs.Rupal Patel,Assistant
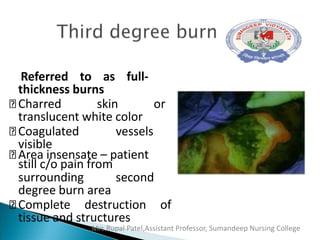
- 11. Referred to as full- thickness burns Charred skin or translucent white color Coagulated vessels visible Area insensate â patient still c/o pain from surrounding second degree burn area Complete destruction of tissue and structures Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
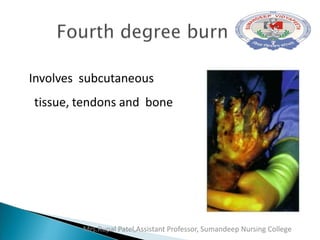
- 12. Involves subcutaneous tissue, tendons and bone Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 13. ï― Rule of Nines: Quick estimate of percent of burn Lund and Browder: More accurate assessment tool Useful chart for children â takes into account the head size proportion. Rule of Palms: Good for estimating small patches of burn wound Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
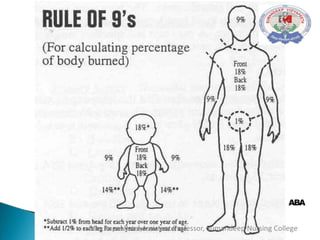
- 14. ï― Head & Neck = 9% ï― Each upper extremity (Arms) = 9% Each lower extremity (Legs) = 18% ï― Anterior trunk= 18% Posterior trunk = 18% Genitalia (perineum) = 1% 17 Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 15. ABA Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 16. 19Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 17. ï― As the primary survey is starting ,give high flow O2 from face mask with a reservior bag. Cooling the burn wound âcold running water for 15- 20 min,avoid making pt hypothermic. Prevent hypothermia-there is disruption to thermoregulation with a significant burn. Insert min 2 peripheral cannula in unburnt skin if possible. Give iv Fluid according to protocol Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 18. ï― Insert urinary catheter in all pts>20% BSA. Fast the pt and insert NG tube for all pts with>20% BSA,all intubated pts,head and neck burns,younger children >10%BSA. Adequate analgesia-IV opioids. Emergency wound management e.g.,cling film or clean non-adhesive dressing. Escharotomy if indicated e.g., circumferential burns around limbs or trunk. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 19. ï― FBC Clotting studies. Electrolytes,renal and liver function. CK( creatin kinase) if suspicion of significant tissue damage. Cross âmatch if early surgery anticipated. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 20. ï― Evidence of possible airway compromise: .burn to head and neck with swelling .stridor,hoarse voice,swollen lips. .singed facial ,nasal or head hairs. . Unconscious . If complex/severe burns which require significant interventions. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 21. ETT used,as chest wall compliance may be reduced resulting in significant leak. Intubation should be performed by experienced individual â failed attempts can create edema and further obstruct the airway Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 22. ï― 4 ml R/L x % burn x body wt. in Kg (eg. 4 x 50% x 45 kg = 9000 ) ï― Â― of calculated fluid is administered in the first 8 hours( 9000/2 =4500 ml) Balance is given over the remaining 16 hours. (4500ml ) Maintain urine output at 0.5 ml/kg/hr. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 23. Surgery and dressings Airway/ventilation Nutrition Antibiotics Miscllaneous Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 24. ï― Escharotomy may be needed for circumferential burns to limbs,neck or trunk. Early surgical debridement of nectrotic tissue is preferred as early grafting is associated with improved outcome. Blood loss during operative sessions can be large. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 25. ï― Early enteral nutrition ideally post pyloric. Aim for a high calorie,high protein intake. Supplement with parenteral if enteral feeding is not well tolerated. Add trace element supplements. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 26. Prophylactic antibiotics are avoided. Fever is universal after a severe burn and doesnât mean infection. Monitor wbc count,check frequent cultures. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 27. ï― Minor changes of dressings are often performed in ward with sedation and analgesia. ICU pts are transferred to operation theater with sedative and analgesic infusions continuing. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College
- 28. Mrs.Rupal Patel,Assistant Professor, Sumandeep Nursing College