




















10929849.ppt
- 1. GIS-K-25 ACUTE APPENDICITIS Appendiceal Mass / Abscess Syahbuddin Harahap Division of Digestive Surgery Department of Surgery Faculty of Medicine University of North Sumatera Adam Malik Hospital
- 2. INTRODUCTION The appendix is : -Wormlike extension of the cecum (vermiform appendix). -Length is 8-10 cm (ranging from 2-20 cm). -Fifth month of gestation -Several lymphoid follicles.
- 3. Etiology: Obstruction of the lumen appendix followed by infection ÔÉòCatarrhal appendicitis. -lymphoid hyperplasia (60% children) -Gastro enteritis -Virus -Acute respiratory infection -Mononucleosis ÔÉòObstructive appendicitis -fecalith 35% adults. -foreign body / parasites (4%) - tumors (1%)
- 4. Pathophysiology Wangensteen proposed 1. Closed loop obstruction 2. Increase in luminal pressure. 3. Exceeds capillary pressure causes mucosal ischemia 4. Luminal bacterial overgrowth and translocation bacteria across the appendiceal wall result : -Inflammation -Edema -Necrosis  perforation occur about 48 hours . If the body successfully walls off the perforation Appendiceal Mass If the perforation is not successfully walled off  Diffuse peritonitis will develop.
- 5. Problem: Appendicitis can mimic several abdominal conditions. ÔÉòLaboratory test ÔÉòImaging investigation Statistics report ÔÉò1 of 5 cases is misdiagnosed ÔÉòNormal appendix is found in 15-40% Emergency appendectomy.(Negative Appendectomy)
- 6. Differential diagnosis of acute appendicitis Surgical • Acute Intestinalobstruction • Intussusception • Acute cholecystitis • Perforated peptic ulcer • Mesenteric adenitis • Acute Meckel's diverticulitis • Acute Pancreatitis Medical • Gastroenteritis • Basal Pneumonia dextra • Terminalileitis Urological • Rightureteric colic • Right pyelonephritis • Urinary tract infection • Right Acute epididymitis Gynaecological • Ectopicpregnancy • Ruptured ovarian follicle • Torted ovarian cyst • Salpingitis/pelvicinflammatory disease
- 7. Differential diagnosis of appendicitis appendicitis can mimic several abdominal conditions.
- 8. Lab Studies: Complete blood cell count A mild elevation of WBCs (ie, >10,000/µL) Urinalysis Mild pyuria relationship of the appendix with the right ureter. Severe pyuria in UTI. For women of childbearing age, Ectopic pregnancy test urin (beta-hCG)
- 9. On physical examination •Lying down •Flexing their hips •The most common symptom of appendicitis is : - Acute abdominal pain. - Epigastric or Periumbilical pain migrating to the right lower quadrant (RLQ) of the abdomen. - Vomiting, nausea, and anorexia - Afebrile or has a low-grade fever , 38 º C •Higher fevers are associated with a perforated appendix
- 10. Special maneuvers McBurney sign McBurney's point it is only the area of greatest tenderness Blumberg sign Rovsing’s Sign Dunphy sign Cough Test Obturator sign Psoas sign Markle sign
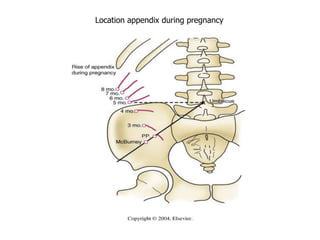
- 11. Location appendix during pregnancy
- 12. INDICATIONS Consider an appendectomy for patients with a history of : •Persistent abdominal pain •Fever •Clinical signs of localized or diffuse peritonitis •Especially if leukocytosis is present.
- 13. Imaging Studies Abdomen plain film: Fecalith within the appendix Urolithiasis right middle third
- 14. MANTRELS SCORE Characteristic Score M = Migration of pain to the RLQ 1 A = Anorexia 1 N = Nausea and vomiting 1 T = Tenderness in RLQ 2 R = Rebound pain 1 E = Elevated temperature 1 L = Leukocytosis 2 S = Shift of WBC to the left 1 Total 10 A score of 7 or more is strongly predictive of acute appendicitis. Alvarado score 1986
- 15. Sonography Advantages of sonography 1. Noninvasiveness, 2. Short acquisition time 3. Lack of radiation exposure 4. Potential for diagnosis of other causes of abdominal pain 5. Pediatric patients 6. Women of childbearing age. 7. Pregnant women normal less than 6 mm
- 16. CT scan -Oral contrast medium -Rectal Gastrografin enema ÔÉòReserved for patients -Uncertain diagnosis -Severe obesity. more than 6 mm
- 17. If the clinical picture is unclear ÔÉòShort period (4-6 h) of watchful waiting ÔÉòUSG / CT scan -May improve diagnostic accuracy ÔÉòWithout a definite diagnosis - return for continued or recurrent symptoms - follow-up examination in 24 hours.
- 18. Complications • Perforation • General Secondary Peritonitis • Appendiceal Mass • Appendiceal Abscess • Pylephlebitis is suppurative thrombophlebitis of the portal venous system • Hepatic absces • Chills • High fever • Jaundice
- 19. TREATMENT Medical therapy ÔÉòResuscitated adequately with fluids . ÔÉòPreoperative prophylactic antibiotics -Acute Appendicitis single agent second-generation cephalosporin. -Perforated appendix triple antibiotic therapy Ampicillin , gentamycin , metronidazol ÔÉòAntibiotic prophylaxis should be administered before every appendectomy. ÔÉòAntibiotic treatment may be stopped. -Becomes afebrile -WBC count normalizes
- 20. Two approaches to appendectomy 1. Open Emergency Appendicectomy ( Appendectomy) 2. Laparoscopic appendectomy ÔÇó If normal appendix removed need to look for: - Meckel's diverticulum - Acute salpingitis - Crohn's disease
- 21. If the body successfully walls off the localized perforation Appendiceal Mass RLQ mass The pain may actually improve. Symptoms do not completely resolve. Still have right lower quadrant pain Decreased appetite Change in bowel habits (eg, diarrhea, constipation) Intermittent low-grade fever.
- 22. Treatment of Appendiceal Mass Nonoperative management Becomes walled off by omentum and ajacent viscera. Initially treated with intravenous broad-spectrum antibiotic Appendiceal Abscess  USG or CT scan -Percutaneous aspiration -Drain placement Intravenous antibiotics are continued until the patient - afebrile for 24 hours - return of normal gastrointestinal function - normal WBC count with a normal differential. At this time, patients are switched to oral antibiotics for a total antibiotic course of 10-14 days. Traditionally, interval appendectomy is performed 6-8 weeks later.
- 24. Acute Appendicitis Appendicitis Perforation