
1 of 1
Downloaded 18 times
Recommended
4 - SAFETY IS THE LIFELINE OF YOUR BUSINESS.pdf
4 - SAFETY IS THE LIFELINE OF YOUR BUSINESS.pdfDwarika Bhushan Sharma
Ã˝
4 - SAFETY IS THE LIFELINE OF YOUR BUSINESS5 - CLOWNS BELONG IN THE CIRCUS & NOT ON THE JOB.pdf
5 - CLOWNS BELONG IN THE CIRCUS & NOT ON THE JOB.pdfDwarika Bhushan Sharma
Ã˝
5 - CLOWNS BELONG IN THE CIRCUS & NOT ON THE JOB3-STOP FALLS, CLEAN UP, PICK UP, WIPE UP.pdf
3-STOP FALLS, CLEAN UP, PICK UP, WIPE UP.pdfDwarika Bhushan Sharma
Ã˝
3-STOP FALLS, CLEAN UP, PICK UP, WIPE UP3-STOP FALLS, CLEAN UP, PICK UP, WIPE UP-STOP FALLS, CLEAN UP, PICK UP, WIPE UP2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASK.pdf
2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASK.pdfDwarika Bhushan Sharma
Ã˝
2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASK 2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASKPRE-START BRIEFING Form # HSEQ - PSB Rev 2 -.docx
PRE-START BRIEFING Form # HSEQ - PSB Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
Project Information:
Project Name:
Location: Supervisor :
Company name : Date:
Task Description:
Before work starts, the following must be in place
Induction Supervision Test Certificates Communication in same language Method Statement Risk Assessment Permit To Work Area Lighting
SELECT HAZARDS SELECT CONTROLS
( Tick to identify the controls in place)
Fall from height Training Access Ladder Access Handrail Edge Protection Secure Ladder Adequate Work Platform Guards for Openings Safety Harness Life Lines
Others( Specify)
Manual Handling Training Check Weight Mechanical Aids Access Route Team Lifting Wrong method Right Method
Power tools Training Color code inspection tag Check Cable Wheel guards Safe plug & sockets Cable Protection Proper Scaffold Cable Overhead Rotatory part guards
Scaffold Scaffold Tag Edge Protection Check Overhead works Access Ladder Adequate Work Platform Weather condition Out riggers Ladder 3 feet above platform Safety Harness
SELECT HAZARDS SELECT CONTROLS
( Tick to identify the controls in place)
Risk Assessment
Lifting Plan Tag Lines Lifting points / hooks Banks man Load stability Check Lifting gear Examination /Inspection Sharp edges protected
Lifting operations Weather/ Wind Speed Ground conditions Exclusion zone Communication Loading/ unloading vehicles Spreader Beams Check Ground conditions Check outriggers Others
Fire Fire Extinguisher Fire Hose Fire Exit Assembly point others
Slip/Trip Clean before you go Barricade the waste Waste Management Clean Access Housekeeping Clean liquid spillage Access signs Maintain access/ Egress
PPE
Safety Harness
Safety Helmet Coveralls Hi vis Jacket Safety Shoe Face Shield Ear Protection
Dust mask Respiratory Equipment Life line/ harness anchorage Hand Gloves Goggles/ Glass
Pre start Briefing done by: Signature:
Reviewed By HSE Manager/ In charge: Signature:
FIRE PREVENTION REQUIREMENTS Form # HSEQ - Rev 2.docx
FIRE PREVENTION REQUIREMENTS Form # HSEQ - Rev 2.docxDwarika Bhushan Sharma
Ã˝
Code of Practice
C.O.P # 01
Fire Prevention Requirements
(Management of Combustible Materials & Electrical Inspections)
Rev. 01, Mar 23
SUB CONTRACTORS HSE CHECKLIST Form # HSEQ - SPSC Rev 2 -.docx
SUB CONTRACTORS HSE CHECKLIST Form # HSEQ - SPSC Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
This document is a sub-contractor pre-start HSE checklist that must be filled out daily before starting any activity. It collects project information, task details including description, location, workers and duration. It also checks that various HSE prerequisites are in place such as safety inductions, risk assessments, PPE availability, inspection of tools and equipment, and that unsafe conditions have been rectified. The sub-contractor must acknowledge that all precautions and control measures have been taken and the workers have been deemed competent to perform the task safely.STORE INSPECTION Form # HSEQ - Form 2 Rev 2.docx
STORE INSPECTION Form # HSEQ - Form 2 Rev 2.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name: Store No.
Location: Contact Person:
Company Name: Arabtec Construction LLC. Date:
Sr. Description Yes No N/A Comments
1. Is access to stores are restricted to authorized personnel only?
2. Are there clear spaces around racks and stacks of stored materials and are adequate gangways provided between them?
3. Are stacks and storage kept clear of light fittings and hot surfaces?
4. Are all stocks of flammable liquids kept in purpose-built flammable storage liquid stores?
5. Are storage areas generally cleaned and tidy?
6. Are flammable liquids kept away from all possible sources of ignition?
7. Emergency exit signs are available in right locations
8. Smoke detectors/fire alarm are visible and accessible.
9. Fire extinguishers are available are serviced regularly
10. Are free standing shelves and cupboards secured for stability?
11. Are heavy items stored at a suitable height?
12. Are chemical containers used for storage suitable and clearly labelled?
13. Is there adequate light in the storage area?
14. Are all small loose items secured in appropriate storage?
15. Are warning notices, prohibiting smoking and naked lights prominently displayed?
16. Others if any:
Remarks:
Inspected by: Signature:
Reviewed by Project Manager/HSE Manager Signature:
WITNESS STATEMENT FORM.docx
WITNESS STATEMENT FORM.docxDwarika Bhushan Sharma
Ã˝
This document records a statement for a project located at an unspecified location. The statement is provided and written by an individual who acknowledges that the information is true to the best of their recollection. The individual provides their name, signature, position and date at the end of the statement.PROJECT LEADER INCIDENT BRIEFING Form # HSEQ - PLIB Rev 2 -.docx
PROJECT LEADER INCIDENT BRIEFING Form # HSEQ - PLIB Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
1. Project Information:
Project Name: Click here to enter text.
Report No.: Click here to enter text.
Project Location: Click here to enter text.
Property No.: Click here to enter text.
‚òê Fatality ‚òê Major Injury ‚òê Minor Injury ‚òê Property Damage ‚òê Environmental ‚òê Other
2. Describe the Incident in detail:
Answer who, what, why, where, when & how in this section: (Attach additional pages if required)
3. Incident Root Causes:
Describe direct, indirect & root cause: (Attach additional pages if required)
4. Key Corrections Taken Immediately after the Incident:
Attach additional pages if more space is required:
5. Key Corrective Actions to Prevent Recurrence:
Describe the corrective actions with timeframe: (Attach additional pages if required)
Corporate Office Remarks:

LIFT SHAFT ENTRY PERMIT Form # HSEQ - LSEP Rev 2 -.docx
LIFT SHAFT ENTRY PERMIT Form # HSEQ - LSEP Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Detail of Surroundings:
Permit Validity:
Time (from): __________Hrs.
Time (To): __________Hrs.
Date:
3. Control Measures: (To be filled by initiator/originator and verified by Evaluator)
Checks Yes-No-NA Checks Yes-No-NA
Method statement & Risk assessment developed, approved & communicated? ‚òê ‚òê ‚òê
Availability of rescue procedure and equipment? ‚òê ‚òê ‚òê
Operatives are trained and competent? ‚òê ‚òê ‚òê
Workplace appropriately illuminated ‚òê ‚òê ‚òê
Any high risk activity associated that requires PTW (i.e. hot work, CSE)? ‚òê ‚òê ‚òê
Forced ventilation provided? ‚òê ‚òê ‚òê
Are all necessary Permit approved and displayed at work location? ‚òê ‚òê ‚òê
Means of communication available? (Mobile, radio etc.) ‚òê ‚òê ‚òê
Safe access / Working Platform provided? ‚òê ‚òê ‚òê
Mandatory/specific good condition PPEs are available ‚òê ‚òê ‚òê
Availability of barricades/protection to prevent unauthorized or accidental entry? ‚òê ‚òê ‚òê
Life Line provided? ‚òê ‚òê ‚òê
Warning signs posted? ‚òê ‚òê ‚òê
Fall Protection equipment (e.g. full body harness) available? ‚òê ‚òê ‚òê
Availability of Fall protection arrangement? ‚òê ‚òê ‚òê
Other(s): ‚òê ‚òê ‚òê
Adequate Lighting provided? ‚òê ‚òê ‚òê
‚òê ‚òê ‚òê
4. Acknowledgement by Initiator and Evaluator:
‚òê Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Time:
‚òê Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity
Evaluator (HSE Team): Designation:
Signature: Time
Comments (if any):
5. Authorization (PM/CM):
Name: Designation:
Signature: Time:
6. Completion/Cancelation of Permit:
‚òê Acknowledge that the area have been restored to a safe and orderly condition.
Initiator Signature: Time:
‚òê Acknowledge that I have checked the area and been restored to a safe and orderly condition.
Evaluator Signature: Time:
LIVE ELECTRICAL WORK PERMIT Form # HSEQ - LEP Rev 2.docx
LIVE ELECTRICAL WORK PERMIT Form # HSEQ - LEP Rev 2.docxDwarika Bhushan Sharma
Ã˝
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Location / Area :
Panel No : Voltage:
Permit Validity:
Time (from): _______Hrs.
Time (To): __________Hrs.
Date:
3. Prerequisites: (To be filled by initiator/originator and verified by Evaluator)
No: Checks Yes-No-NA Checks Yes-No-NA
ENERGIZATION (“Power On”) ISOLATION (“Power Off”)
1. Safety tool box briefing done. ‚òê ‚òê ‚òê
Method statement/Risk assessment in place. ‚òê ‚òê ‚òê
2. Authorized personnel / operators available. ‚òê ‚òê ‚òê
Authorized personnel / operators available. ‚òê ‚òê ‚òê
3. Method statement/Risk assessment in place. ‚òê ‚òê ‚òê
Adjacent live areas protected. ‚òê ‚òê ‚òê
4. Safety Barriers in place and safety signage Displayed. ‚òê ‚òê ‚òê
PPE available, high voltage rubber gloves, Safety goggles and floor mat. ‚òê ‚òê ‚òê
5. Working area is well lighted. ‚òê ‚òê ‚òê
Isolation/Lock-out in place. ‚òê ‚òê ‚òê
6. Electrical instruments are available for any Purpose. ‚òê ‚òê ‚òê
Electrical circuits “proved” by calibrated Instrument and found out to be no power. ☐ ☐ ☐
7. Correct PPE available, high voltage rubber Gloves, safety goggles and floor mat. ‚òê ‚òê ‚òê
Unauthorized workers are cleared from the Area. ‚òê ‚òê ‚òê
8. Approved WIR for installation, testing and Termination are attached to the permit. ‚òê ‚òê ‚òê
Standby operatives in the event of contact With live circuits. ‚òê ‚òê ‚òê
9. Emergency light (Flashlight) available. ‚òê ‚òê ‚òê
Emergency light (Flashlight) available. ‚òê ‚òê ‚òê
10. Is live work absolutely necessary? ‚òê ‚òê ‚òê
Emergency response plan available ‚òê ‚òê ‚òê
11. Unauthorized workers are cleared from the area.
‚òê ‚òê ‚òê
Other ( Specify): ‚òí ‚òê ‚òê
12. Power cable route from panel board to plant & equipment has been checked ‚òê ‚òê ‚òê
13 Emergency response plan available ‚òê ‚òê ‚òê
14 Other ( Specify): ‚òê ‚òê ‚òê
4. Acknowledgement by Initiator and Evaluator:
‚òê Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Date /Time:
‚òê Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity
Evaluator (HSE Team): Designation:
Signature: Date /Time
Comments (if any):
5. Authorization (PM/CM):
Name: Designation:
Signature: Date /Time:
6. Completion/Cancelation of Permit:
‚òê Acknowledge that the area have been restored to a safe and orderly condition.
Initiator Signature: Time:
‚òê Acknowledge that I have checked the area and been restored to a safe and orderly condition.
Evaluator Signature: Time:
MOBILE PLANT REGISTER Form # HSEQ - MPR Rev 3.docx
MOBILE PLANT REGISTER Form # HSEQ - MPR Rev 3.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name:
Date: Location:
Sr. Equipment type / Name Registration No & Exp Date Company Name
Operator Name / Mb. No Operator Third party competency certificate expiry date Operator License expiry date Equipment & Plant 3rd Party Inspection Certificate expiry date SWL / Capacity Signalman /Rigger name & TPC Exp Comment
1
2
3
4
5
6
7
8
9
10.
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge: Signature:
LABOR ACCOMMODATION CHECKLIST Form # HSEQ - LAC Rev 2.docx
LABOR ACCOMMODATION CHECKLIST Form # HSEQ - LAC Rev 2.docxDwarika Bhushan Sharma
Ã˝
This 5-page document is a checklist for inspecting labour accommodation on a weekly basis. It contains over 100 questions across various categories including access/egress, housekeeping, septic tanks, food preparation, living quarters, firefighting, emergency procedures, first aid, record keeping, environment, and civil defence requirements. Inspectors are to verify that accommodation meets standards for safety, sanitation, emergency preparedness and regulatory compliance by completing the checklist and noting any needed corrective actions or due dates.INCIDENT INVESTIGATION REPORT Form # HSEQ - IIR Rev 9 -.docx
INCIDENT INVESTIGATION REPORT Form # HSEQ - IIR Rev 9 -.docxDwarika Bhushan Sharma
Ã˝
INCIDENT INVESTIGATION REPORT
(To be submitted to the HSEQ Corporate Office within 7 days of incident.)
1. Project Information:
Project Name: Click here to enter text.
Report No.: Click here to enter text.
Project Location: Click here to enter text.
Property No.: Click here to enter text.
‚òê Fatality ‚òê Major Incident ‚òê Minor Incident
2. Describe the Incident in detail:
Answer who, what, why, where, when & how in this section: (Attach additional pages if required)
Click here to enter text.
‚òê Photos Attached
3. Incident Root Causes:
Describe direct, indirect & root cause: (Attach additional pages if required)
Click here to enter text.
4. Key Corrective Actions to Prevent Recurrence:
Describe the corrective actions with timeframe: (Attach additional pages if required)
Click here to enter text.
5. Key Corrections Taken Immediately after the Incident:
Attach additional pages if more space is required:
Click here to enter text.
6. Witnesses:
I declare that I witnessed the incident and the information provided above is true, correct and complete.
No. Name Designation Signature Date
1. Click here to enter text.
Click here to enter text.
Click here to enter text.
2. Click here to enter text.
Click here to enter text.
Click here to enter text.
7. Incident Information:
Initial Incident Report No.: Click here to enter text.
Date Reported: Click here to enter text.
Date of Incident: Click here to enter text.
Time of Incident: Click here to enter text.
Type of Incident: ‚òê Near Miss
‚òê Major Environmental Incident
‚òê Serious Dangerous Occurrence
‚òê Equipment / Property Damage
‚òê Medical Treatment Case (MTC)
‚òê Restricted Work Case (RWC)
‚òê Lost Workday Case (LWC)
‚òê Serious Occupational Illness/Disease
‚òê Class 1 Injuries
‚òê Permanent Partial Disability (PPD)
‚òê Permanent Total Disability (PTD)
‚òê Fatality (F)
Recordkeeping: ‚òê Reportable ‚òê Recordable
Incident Location on Site: Click here to enter text.
Applicable Reports: ‚òê Police
‚òê Medical
‚òê Other (Specify)
Click here to enter text.
Attached: ‚òê Yes ‚òê No
‚òê Yes ‚òê No
‚òê Yes ‚òê No
8. Injured Person’s Personal Details:
In case of an incident with more than one injured person, complete the information for each person using separate forms.
Name: Click here to enter text.
Occupation: Click here to enter text.
Company: Click here to enter text.
MB / Oracle No.: Click here to enter text.
Nationality: Click here to enter text.
Date of Birth: Click here to enter text.
Passport Number: Click here to enter text.
Length of Service: Click here to enter text.
Gender: ‚òê Male ‚òê Female
Labour Card No.: Click here to enter text.
9. Incident Causes Details: To be supported with factual evidence
Immediate Cause
(Unsafe Acts) ‚òê Failure to secure
‚òê Failure to warn
‚òê Removing / Defeating Safety Devices
‚òêHSE INDUCTION Form # HSEQ - HSEI Rev 2 -.doc
HSE INDUCTION Form # HSEQ - HSEI Rev 2 -.docDwarika Bhushan Sharma
Ã˝
HSE INDUCTION
(Workers)
Name: _________________________________ Trade: ____________________________
M.B. No./Company Name : ________________
Date of Joining: __________________________
SL. N SUBJECT ON INDUCTION PREVIOUS SAFETY EXPOSURE FURTHER SAFETY TRAINING NEED ANALYSIS
1. Introduction Safety Requirements
2. Working Safety is of Primary Importance
3. General Safety Rules
4. Basic Safety Requirements
5. House Keeping
6. Health, Hygiene & Welfare Facilities
7. Fire Extinguisher / Fire Fighting
8. Emergency Procedure
9. Safety Violations & Penalty
10. Safety Award
11. Manual Handling
Induction Given By: Name: ___________________________
Designation: ___________________________
HSE WARNING LETTER-DISCIPLINARY NOTICE Form # HSEQ - HSEWL Rev 6.doc
HSE WARNING LETTER-DISCIPLINARY NOTICE Form # HSEQ - HSEWL Rev 6.docDwarika Bhushan Sharma
Ã˝
1st Warning 0 Ref. No. ______________
2nd Warning 0
3rd Warning 0
4th Warning 0 Date: ________________
Employee’s Name : ______________________________________ M.B No. : __________
Occupation : _____________________________________________________________________
Location / Project Site: _____________________________________________________________________
You have committed the following HSE violation/s:
………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………….….
The employee is hereby warned that if the violation is repeated further disciplinary action can be
taken as per the company Code of Conduct.
ORIGINATOR APPROVED BY (MANAGER IN CHARGE / ARABTEC HSEQ & ORG. RISK Manager)
Name: _______________________________ Name: _____________________________
Designation: _______________________________ Designation: _____________________________
Signature:
_______________________________ Signature:
_____________________________
Employee Acknowledgement:
I the undersigned have received this Safety warning letter / disciplinary notice and I admit that I have understood the contents.
0 Received on: ………………………….. (Date) Signature: ………………………………..…..
OFFICE PORTA CABIN INSPECTION Form # HSEQ - OPC Rev 2.docx
OFFICE PORTA CABIN INSPECTION Form # HSEQ - OPC Rev 2.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name: Porta Cabin No:
Location: Contact Person:
Company Name: Date :
Sr. Description Yes No N/A Comments
1. Emergency exit signs are available in right locations
2. Fire alarms and fire extinguishers are visible and accessible.
3. Fire doors (e.g. in stairways) are kept closed unless equipped with automatic closing device
4. Fire extinguishers are serviced regularly
5. Corridors and stairways are kept free of obstruction
6. Fire escape/ evacuation plan available and posted
7. First aid box available
8. Floor surfaces are kept dry and free of slip hazards
9. Electrical cords and plugs are in good condition with proper Grounding
10. Kitchen equipment checked
11. Fire blanket available in the pantry
12. Heat detector available in the pantry
13. Toilets floor clean and dry
14. Are staff trained to use Fire Extinguishers
15. Hand wash/ soap solution available in the toilet
16. Civil Defense or Authority approval
17. Others if any:
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
MEDICAL REPORT FORM Form # HSEQ - MRF Rev 3 -.docx
MEDICAL REPORT FORM Form # HSEQ - MRF Rev 3 -.docxDwarika Bhushan Sharma
Ã˝
MEDICAL REPORT FORM
Day _____________
Date ____________
Time ____________
To: _________________________________________________________________________________________________________
Dear Sir,
We would kindly request you to give necessary treatment to our following employee who had met with an accident and provide us with your diagnosis.
Name of injured __________________________________________________________ Age ( ) years.
Occupation __________________________________________________________ M.B. No. _______________________________
Date of Accident ____________________________________________ Time of Accident __________________________________
Place of Accident (Project Name) _______________________________ Location _________________________________________
Nature of Accident ____________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
First Aider Name: ________________________________ SE Manager/Incharge: ________________________________
Signature: ________________________________ Signature: ________________________________
(If Medical Certificate is attached, this portion is not required.)
MEDICAL REPORT
Nature and extent of Accident / Injury____________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Fit for duty___________________________________________________________________________________________________
Unfit for duty_________________________________________________________________________________________________
Remarks_____________________________________________________________________________________________________
____________________________________________________________________________________________________________
Signature of Medical Officer Date _______________
LIFTING TACKLE VISUAL INSPECTION & REGISTER Form # HSEQ - LTVIR Rev 3.docx
LIFTING TACKLE VISUAL INSPECTION & REGISTER Form # HSEQ - LTVIR Rev 3.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name:
Company Name: Date :
ID NO TYPE OF LIFTING GEARS LOCATION VISUAL INSPECTION THIRD PARTY INSPECTION VALID TILL MONTHLY COLOUR CODE
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
FULL BODY HARNESS INSPECTION RECORD Form # HSEQ - FBHIR Rev 2.docx
FULL BODY HARNESS INSPECTION RECORD Form # HSEQ - FBHIR Rev 2.docxDwarika Bhushan Sharma
Ã˝
Harness Checklist
Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Remarks
Shoulder Straps
Chest & Back Straps
Waist Straps
Back D-Ring
Shoulder Adjustment
Legible Label
Shoulder Straps
Chest & Back Straps
Waist Straps
Leg Straps
Cuts
Burns
Holes
Deterioration
Corrosive/ worn out
Color code
Others (Specify)
Project Information
Project Name: Location:
Company name : Date:
Remarks:
Inspector Name: Signature:
Reviewed By HSE Manager / Incharge Signature:
GENERAL SITE SAFETY RULES Form # HSEQ - Rev 2.docx
GENERAL SITE SAFETY RULES Form # HSEQ - Rev 2.docxDwarika Bhushan Sharma
Ã˝
Always wear proper personal protective equipment and inspect and maintain it. You are responsible for your own safety and others, so report any unsafe acts or conditions and avoid taking shortcuts or engaging in horseplay or fights. Communicate risks and follow all safety procedures and instructions.HAZARDOUS SUBSTANCE CHECKLIST Form # HSEQ - HSC Rev 2 -.docx
HAZARDOUS SUBSTANCE CHECKLIST Form # HSEQ - HSC Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name:
Location:
Company Name: Date :
Sl. No Description Yes No N/A Comments
1. Properly stored, labeled, ventilated, isolated, Log and suitable signs displayed.
2. Material Data Safety Sheet (MSDS) available, and communicated to concerned personnel.
3. Adequate/ Sufficient firefighting equipment are in place.
4. Emergency escape and breathing apparatus available, tested and in good condition.
5. Hazardous substances containers/drums have eligible labeling and protected from leakages or spillage.
6. Personnel must be trained in chemical handling.
7. Emergency control plan must be made available, spillage control kits must be available.
8. Empty hazardous substances containers, drums and receptacles should be properly maintained and controlled.
9. Expired chemicals are logged, segregated and disposed properly
10. Others Specify
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
CONCRETE PUMP & EXTENSION PIPELINE Form # HSEQ - CPC Rev 2.docx
CONCRETE PUMP & EXTENSION PIPELINE Form # HSEQ - CPC Rev 2.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name: Concrete Pump Reg. No:
Location: Operators Name:
Company Name: Date :
Sr. Description Yes No N/A Comments
1. Concrete Pump 3rd Party Certificate & Registration
2. Sonographic test of all pipes
3. Calibration of all the pressure gauges
4. Operator’s Competency Certificate & Driver’s License
5. Safe distance from the edge of the excavation
6. Outrigger pads are free from damage
7. Outriggers are level
8. Reverse alarm and beacon light are operational
9. Whip arrester on the pipes and pump
10. Safe access for concrete mixer to the area (In/Out)
11. Area properly barricaded and signage posted
12. Hydraulic Oil / Diesel Leakage
13. Extension Pipeline - Free from damage
14. Extension Pipeline -Locking pin in every connection
15. Extension Pipeline - Adequately supported & secured
16. Spillage control measure in place
17. Other accessories e.g. spider pacing boom 3rd party certificate
18. Static pumps positioned properly
19. Static pumps – concrete pipes fixed on structure as per design
20. Concrete pipes coupler pins provided
21. Concrete pipes on floor – away from scaffolds/ formworks
22. Competent banks man and supervision provided
23. Others (Specify)
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
Noted by Project Leader Signature:
BEHAVIORAL OBSERVATION Form # HSEQ BO Rev.0.docx
BEHAVIORAL OBSERVATION Form # HSEQ BO Rev.0.docxDwarika Bhushan Sharma
Ã˝
Project Behavioral Observation Form
Process Observed
Works Package
Subcontractor / CName
Date _ _ /_ _ /_ _ Time from ______ to ______ Duration Mins _____
Checklist attached ‚òê
Video ‚òê
Photo (s) ‚òê
Observation Summary (Ref checklist for details)
Safe ‚òê
Unsafe Acts ‚òê
Safe ‚òê
Unsafe conditions ‚òê
Status:
A. All activities conducted in a safe manner ‚òê
No negative observations
B. Generally conducted in a safe manner ‚òê
Some aspects of the process require improvement
C. Partially conducted in a safe manner ‚òê
One aspect of a task needs improvement
D. Some individual lapses ‚òê
One person working unsafely part of the time
E. Generally conducted in unsafe manner ‚òê
More than one person working unsafely
ATC Engineer-in-charge Supervisor
Follow up Action
‚òê
Analysed by HSE Manager and responsible person _________________
‚òê
Reported / shown to team observed
‚òê
Recommended Action
‚òê
Follow up recommendation
FIRE PREVENTION CHECKLIST Form # HSEQ - FPC Rev 2 -.docx
FIRE PREVENTION CHECKLIST Form # HSEQ - FPC Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
SR. TITLE YES NO N/A Comments
1 FIRE PROTECTION EQUIPMENT
1.1 Are adequate fire-fighting equipment and sufficient extinguishing agents available and operative at all times? ÔÇ£
ÔÇ£
ÔÇ£
1.2 Have workers been oriented on their correct use and operation? ÔÇ£
ÔÇ£
ÔÇ£
1.3 Are portable fire extinguishers of sufficient capacity (at least 20 lbs.) and type available and strategically positioned near hazardous work such that the travel distance to the nearest unit is no greater than 15 meters? ÔÇ£
ÔÇ£
ÔÇ£
1.4 Are regular checks undertaken to make sure that the equipment is not missing or damaged? ÔÇ£
ÔÇ£
ÔÇ£
1.5 Is a fully operational yard hydrant/Fire Hose reel system available prior to start of construction (excluding foundation work) and during the entire construction period?
Where street hydrants are not available, are temporary hydrants provided? ÔÇ£
ÔÇ£
ÔÇ£
1.6 Is a waterline extended as soon as possible behind construction to supplement the Fire Extinguishers placed throughout the construction area? ÔÇ£
ÔÇ£
ÔÇ£
1.7 Are permanent standpipes extended as close as possible behind construction to allow use in case of fire? ÔÇ£
ÔÇ£
ÔÇ£
1.8 Are fully operative standpipes (wet risers) installed up to one level below the highest current work level and are sealed by temporary end caps? ÔÇ£
ÔÇ£
ÔÇ£
1.9 (The following is a less stringent alternative to Item 8 above)
Where construction involves buildings more than 23 meters high, are fully operative standpipes (wet risers) available not less than
3 levels below the highest level under construction.
Where the provision of wet risers does not impede structural work, are they provided to the level below the highest level under construction? ÔÇ£
ÔÇ£
ÔÇ£
1.10 Are the cabinets containing hose reels and portable fire extinguishers inspected at regular intervals but at least twice a week by competent persons? ÔÇ£
ÔÇ£
ÔÇ£
1.11 Are hydrants and standpipes including fire water supply system designed and installed in compliance with UAE Fire and Life safety COP and according to the relevant internationally recognized codes and standards, e.g., NFPA, FM, etc.? ÔÇ£
ÔÇ£
ÔÇ£
1.12 Is the fire water supply at the site available at the required volume and pressure? ÔÇ£
ÔÇ£
ÔÇ£
1.13 Is storage of any material within 3 meters of fire hydrants/Fire Hose reels strictly prohibited? Is access to the outlets unobstructed? ÔÇ£
ÔÇ£
ÔÇ£
2 COMPARTEMENTATION / SEGMENTATION YES NO N/A COMMENTS
2.1 Are fire compartments as required by local regulations installed as soon as possible after the removal of formwork? ÔÇ£
ÔÇ£
ÔÇ£
2.2 Are openings for lift shafts, service ducts and other voids provisionally closed as soon as possible but not later than at the commencement of fit-out work? ÔÇ£
ÔÇ£
ÔÇ£
3 FIRE PREVENTION : HOT WORK MANAGEMENT YES NO N/A COMMENTS
3.1 Is a “permit to work” system being implemented for all parties engaged in “hot work” of any kind such as but not limited to
– grinding, cutting or welding operations,
– use of blow lamps and torches,
– application of hot bitumen
or any other heat-proCOLD WORK PERMIT Form # HSEQ - CWP Rev 2.docx
COLD WORK PERMIT Form # HSEQ - CWP Rev 2.docxDwarika Bhushan Sharma
Ã˝
This cold work permit document is a 2-page form used to request and approve cold work. It lists the job location and description, tools and materials used, potential hazards, precautions needed, and protective equipment. The form requires signatures from the permit requester, acceptor, issuer, and other parties to hand over responsibility between shifts, declare work completion, ensure the site is left safely, and sign off and cancel the permit.

More Related Content
More from Dwarika Bhushan Sharma (20)
WITNESS STATEMENT FORM.docx
WITNESS STATEMENT FORM.docxDwarika Bhushan Sharma
Ã˝
This document records a statement for a project located at an unspecified location. The statement is provided and written by an individual who acknowledges that the information is true to the best of their recollection. The individual provides their name, signature, position and date at the end of the statement.PROJECT LEADER INCIDENT BRIEFING Form # HSEQ - PLIB Rev 2 -.docx
PROJECT LEADER INCIDENT BRIEFING Form # HSEQ - PLIB Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
1. Project Information:
Project Name: Click here to enter text.
Report No.: Click here to enter text.
Project Location: Click here to enter text.
Property No.: Click here to enter text.
‚òê Fatality ‚òê Major Injury ‚òê Minor Injury ‚òê Property Damage ‚òê Environmental ‚òê Other
2. Describe the Incident in detail:
Answer who, what, why, where, when & how in this section: (Attach additional pages if required)
3. Incident Root Causes:
Describe direct, indirect & root cause: (Attach additional pages if required)
4. Key Corrections Taken Immediately after the Incident:
Attach additional pages if more space is required:
5. Key Corrective Actions to Prevent Recurrence:
Describe the corrective actions with timeframe: (Attach additional pages if required)
Corporate Office Remarks:
LIFT SHAFT ENTRY PERMIT Form # HSEQ - LSEP Rev 2 -.docx
LIFT SHAFT ENTRY PERMIT Form # HSEQ - LSEP Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Detail of Surroundings:
Permit Validity:
Time (from): __________Hrs.
Time (To): __________Hrs.
Date:
3. Control Measures: (To be filled by initiator/originator and verified by Evaluator)
Checks Yes-No-NA Checks Yes-No-NA
Method statement & Risk assessment developed, approved & communicated? ‚òê ‚òê ‚òê
Availability of rescue procedure and equipment? ‚òê ‚òê ‚òê
Operatives are trained and competent? ‚òê ‚òê ‚òê
Workplace appropriately illuminated ‚òê ‚òê ‚òê
Any high risk activity associated that requires PTW (i.e. hot work, CSE)? ‚òê ‚òê ‚òê
Forced ventilation provided? ‚òê ‚òê ‚òê
Are all necessary Permit approved and displayed at work location? ‚òê ‚òê ‚òê
Means of communication available? (Mobile, radio etc.) ‚òê ‚òê ‚òê
Safe access / Working Platform provided? ‚òê ‚òê ‚òê
Mandatory/specific good condition PPEs are available ‚òê ‚òê ‚òê
Availability of barricades/protection to prevent unauthorized or accidental entry? ‚òê ‚òê ‚òê
Life Line provided? ‚òê ‚òê ‚òê
Warning signs posted? ‚òê ‚òê ‚òê
Fall Protection equipment (e.g. full body harness) available? ‚òê ‚òê ‚òê
Availability of Fall protection arrangement? ‚òê ‚òê ‚òê
Other(s): ‚òê ‚òê ‚òê
Adequate Lighting provided? ‚òê ‚òê ‚òê
‚òê ‚òê ‚òê
4. Acknowledgement by Initiator and Evaluator:
‚òê Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Time:
‚òê Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity
Evaluator (HSE Team): Designation:
Signature: Time
Comments (if any):
5. Authorization (PM/CM):
Name: Designation:
Signature: Time:
6. Completion/Cancelation of Permit:
‚òê Acknowledge that the area have been restored to a safe and orderly condition.
Initiator Signature: Time:
‚òê Acknowledge that I have checked the area and been restored to a safe and orderly condition.
Evaluator Signature: Time:
LIVE ELECTRICAL WORK PERMIT Form # HSEQ - LEP Rev 2.docx
LIVE ELECTRICAL WORK PERMIT Form # HSEQ - LEP Rev 2.docxDwarika Bhushan Sharma
Ã˝
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Location / Area :
Panel No : Voltage:
Permit Validity:
Time (from): _______Hrs.
Time (To): __________Hrs.
Date:
3. Prerequisites: (To be filled by initiator/originator and verified by Evaluator)
No: Checks Yes-No-NA Checks Yes-No-NA
ENERGIZATION (“Power On”) ISOLATION (“Power Off”)
1. Safety tool box briefing done. ‚òê ‚òê ‚òê
Method statement/Risk assessment in place. ‚òê ‚òê ‚òê
2. Authorized personnel / operators available. ‚òê ‚òê ‚òê
Authorized personnel / operators available. ‚òê ‚òê ‚òê
3. Method statement/Risk assessment in place. ‚òê ‚òê ‚òê
Adjacent live areas protected. ‚òê ‚òê ‚òê
4. Safety Barriers in place and safety signage Displayed. ‚òê ‚òê ‚òê
PPE available, high voltage rubber gloves, Safety goggles and floor mat. ‚òê ‚òê ‚òê
5. Working area is well lighted. ‚òê ‚òê ‚òê
Isolation/Lock-out in place. ‚òê ‚òê ‚òê
6. Electrical instruments are available for any Purpose. ‚òê ‚òê ‚òê
Electrical circuits “proved” by calibrated Instrument and found out to be no power. ☐ ☐ ☐
7. Correct PPE available, high voltage rubber Gloves, safety goggles and floor mat. ‚òê ‚òê ‚òê
Unauthorized workers are cleared from the Area. ‚òê ‚òê ‚òê
8. Approved WIR for installation, testing and Termination are attached to the permit. ‚òê ‚òê ‚òê
Standby operatives in the event of contact With live circuits. ‚òê ‚òê ‚òê
9. Emergency light (Flashlight) available. ‚òê ‚òê ‚òê
Emergency light (Flashlight) available. ‚òê ‚òê ‚òê
10. Is live work absolutely necessary? ‚òê ‚òê ‚òê
Emergency response plan available ‚òê ‚òê ‚òê
11. Unauthorized workers are cleared from the area.
‚òê ‚òê ‚òê
Other ( Specify): ‚òí ‚òê ‚òê
12. Power cable route from panel board to plant & equipment has been checked ‚òê ‚òê ‚òê
13 Emergency response plan available ‚òê ‚òê ‚òê
14 Other ( Specify): ‚òê ‚òê ‚òê
4. Acknowledgement by Initiator and Evaluator:
‚òê Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Date /Time:
‚òê Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity
Evaluator (HSE Team): Designation:
Signature: Date /Time
Comments (if any):
5. Authorization (PM/CM):
Name: Designation:
Signature: Date /Time:
6. Completion/Cancelation of Permit:
‚òê Acknowledge that the area have been restored to a safe and orderly condition.
Initiator Signature: Time:
‚òê Acknowledge that I have checked the area and been restored to a safe and orderly condition.
Evaluator Signature: Time:
MOBILE PLANT REGISTER Form # HSEQ - MPR Rev 3.docx
MOBILE PLANT REGISTER Form # HSEQ - MPR Rev 3.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name:
Date: Location:
Sr. Equipment type / Name Registration No & Exp Date Company Name
Operator Name / Mb. No Operator Third party competency certificate expiry date Operator License expiry date Equipment & Plant 3rd Party Inspection Certificate expiry date SWL / Capacity Signalman /Rigger name & TPC Exp Comment
1
2
3
4
5
6
7
8
9
10.
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge: Signature:
LABOR ACCOMMODATION CHECKLIST Form # HSEQ - LAC Rev 2.docx
LABOR ACCOMMODATION CHECKLIST Form # HSEQ - LAC Rev 2.docxDwarika Bhushan Sharma
Ã˝
This 5-page document is a checklist for inspecting labour accommodation on a weekly basis. It contains over 100 questions across various categories including access/egress, housekeeping, septic tanks, food preparation, living quarters, firefighting, emergency procedures, first aid, record keeping, environment, and civil defence requirements. Inspectors are to verify that accommodation meets standards for safety, sanitation, emergency preparedness and regulatory compliance by completing the checklist and noting any needed corrective actions or due dates.INCIDENT INVESTIGATION REPORT Form # HSEQ - IIR Rev 9 -.docx
INCIDENT INVESTIGATION REPORT Form # HSEQ - IIR Rev 9 -.docxDwarika Bhushan Sharma
Ã˝
INCIDENT INVESTIGATION REPORT
(To be submitted to the HSEQ Corporate Office within 7 days of incident.)
1. Project Information:
Project Name: Click here to enter text.
Report No.: Click here to enter text.
Project Location: Click here to enter text.
Property No.: Click here to enter text.
‚òê Fatality ‚òê Major Incident ‚òê Minor Incident
2. Describe the Incident in detail:
Answer who, what, why, where, when & how in this section: (Attach additional pages if required)
Click here to enter text.
‚òê Photos Attached
3. Incident Root Causes:
Describe direct, indirect & root cause: (Attach additional pages if required)
Click here to enter text.
4. Key Corrective Actions to Prevent Recurrence:
Describe the corrective actions with timeframe: (Attach additional pages if required)
Click here to enter text.
5. Key Corrections Taken Immediately after the Incident:
Attach additional pages if more space is required:
Click here to enter text.
6. Witnesses:
I declare that I witnessed the incident and the information provided above is true, correct and complete.
No. Name Designation Signature Date
1. Click here to enter text.
Click here to enter text.
Click here to enter text.
2. Click here to enter text.
Click here to enter text.
Click here to enter text.
7. Incident Information:
Initial Incident Report No.: Click here to enter text.
Date Reported: Click here to enter text.
Date of Incident: Click here to enter text.
Time of Incident: Click here to enter text.
Type of Incident: ‚òê Near Miss
‚òê Major Environmental Incident
‚òê Serious Dangerous Occurrence
‚òê Equipment / Property Damage
‚òê Medical Treatment Case (MTC)
‚òê Restricted Work Case (RWC)
‚òê Lost Workday Case (LWC)
‚òê Serious Occupational Illness/Disease
‚òê Class 1 Injuries
‚òê Permanent Partial Disability (PPD)
‚òê Permanent Total Disability (PTD)
‚òê Fatality (F)
Recordkeeping: ‚òê Reportable ‚òê Recordable
Incident Location on Site: Click here to enter text.
Applicable Reports: ‚òê Police
‚òê Medical
‚òê Other (Specify)
Click here to enter text.
Attached: ‚òê Yes ‚òê No
‚òê Yes ‚òê No
‚òê Yes ‚òê No
8. Injured Person’s Personal Details:
In case of an incident with more than one injured person, complete the information for each person using separate forms.
Name: Click here to enter text.
Occupation: Click here to enter text.
Company: Click here to enter text.
MB / Oracle No.: Click here to enter text.
Nationality: Click here to enter text.
Date of Birth: Click here to enter text.
Passport Number: Click here to enter text.
Length of Service: Click here to enter text.
Gender: ‚òê Male ‚òê Female
Labour Card No.: Click here to enter text.
9. Incident Causes Details: To be supported with factual evidence
Immediate Cause
(Unsafe Acts) ‚òê Failure to secure
‚òê Failure to warn
‚òê Removing / Defeating Safety Devices
‚òêHSE INDUCTION Form # HSEQ - HSEI Rev 2 -.doc
HSE INDUCTION Form # HSEQ - HSEI Rev 2 -.docDwarika Bhushan Sharma
Ã˝
HSE INDUCTION
(Workers)
Name: _________________________________ Trade: ____________________________
M.B. No./Company Name : ________________
Date of Joining: __________________________
SL. N SUBJECT ON INDUCTION PREVIOUS SAFETY EXPOSURE FURTHER SAFETY TRAINING NEED ANALYSIS
1. Introduction Safety Requirements
2. Working Safety is of Primary Importance
3. General Safety Rules
4. Basic Safety Requirements
5. House Keeping
6. Health, Hygiene & Welfare Facilities
7. Fire Extinguisher / Fire Fighting
8. Emergency Procedure
9. Safety Violations & Penalty
10. Safety Award
11. Manual Handling
Induction Given By: Name: ___________________________
Designation: ___________________________
HSE WARNING LETTER-DISCIPLINARY NOTICE Form # HSEQ - HSEWL Rev 6.doc
HSE WARNING LETTER-DISCIPLINARY NOTICE Form # HSEQ - HSEWL Rev 6.docDwarika Bhushan Sharma
Ã˝
1st Warning 0 Ref. No. ______________
2nd Warning 0
3rd Warning 0
4th Warning 0 Date: ________________
Employee’s Name : ______________________________________ M.B No. : __________
Occupation : _____________________________________________________________________
Location / Project Site: _____________________________________________________________________
You have committed the following HSE violation/s:
………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………….….
The employee is hereby warned that if the violation is repeated further disciplinary action can be
taken as per the company Code of Conduct.
ORIGINATOR APPROVED BY (MANAGER IN CHARGE / ARABTEC HSEQ & ORG. RISK Manager)
Name: _______________________________ Name: _____________________________
Designation: _______________________________ Designation: _____________________________
Signature:
_______________________________ Signature:
_____________________________
Employee Acknowledgement:
I the undersigned have received this Safety warning letter / disciplinary notice and I admit that I have understood the contents.
0 Received on: ………………………….. (Date) Signature: ………………………………..…..
OFFICE PORTA CABIN INSPECTION Form # HSEQ - OPC Rev 2.docx
OFFICE PORTA CABIN INSPECTION Form # HSEQ - OPC Rev 2.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name: Porta Cabin No:
Location: Contact Person:
Company Name: Date :
Sr. Description Yes No N/A Comments
1. Emergency exit signs are available in right locations
2. Fire alarms and fire extinguishers are visible and accessible.
3. Fire doors (e.g. in stairways) are kept closed unless equipped with automatic closing device
4. Fire extinguishers are serviced regularly
5. Corridors and stairways are kept free of obstruction
6. Fire escape/ evacuation plan available and posted
7. First aid box available
8. Floor surfaces are kept dry and free of slip hazards
9. Electrical cords and plugs are in good condition with proper Grounding
10. Kitchen equipment checked
11. Fire blanket available in the pantry
12. Heat detector available in the pantry
13. Toilets floor clean and dry
14. Are staff trained to use Fire Extinguishers
15. Hand wash/ soap solution available in the toilet
16. Civil Defense or Authority approval
17. Others if any:
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
MEDICAL REPORT FORM Form # HSEQ - MRF Rev 3 -.docx
MEDICAL REPORT FORM Form # HSEQ - MRF Rev 3 -.docxDwarika Bhushan Sharma
Ã˝
MEDICAL REPORT FORM
Day _____________
Date ____________
Time ____________
To: _________________________________________________________________________________________________________
Dear Sir,
We would kindly request you to give necessary treatment to our following employee who had met with an accident and provide us with your diagnosis.
Name of injured __________________________________________________________ Age ( ) years.
Occupation __________________________________________________________ M.B. No. _______________________________
Date of Accident ____________________________________________ Time of Accident __________________________________
Place of Accident (Project Name) _______________________________ Location _________________________________________
Nature of Accident ____________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
First Aider Name: ________________________________ SE Manager/Incharge: ________________________________
Signature: ________________________________ Signature: ________________________________
(If Medical Certificate is attached, this portion is not required.)
MEDICAL REPORT
Nature and extent of Accident / Injury____________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Fit for duty___________________________________________________________________________________________________
Unfit for duty_________________________________________________________________________________________________
Remarks_____________________________________________________________________________________________________
____________________________________________________________________________________________________________
Signature of Medical Officer Date _______________
LIFTING TACKLE VISUAL INSPECTION & REGISTER Form # HSEQ - LTVIR Rev 3.docx
LIFTING TACKLE VISUAL INSPECTION & REGISTER Form # HSEQ - LTVIR Rev 3.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name:
Company Name: Date :
ID NO TYPE OF LIFTING GEARS LOCATION VISUAL INSPECTION THIRD PARTY INSPECTION VALID TILL MONTHLY COLOUR CODE
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
‚òê OK ‚òê Not OK
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
FULL BODY HARNESS INSPECTION RECORD Form # HSEQ - FBHIR Rev 2.docx
FULL BODY HARNESS INSPECTION RECORD Form # HSEQ - FBHIR Rev 2.docxDwarika Bhushan Sharma
Ã˝
Harness Checklist
Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Sl. No
………. Remarks
Shoulder Straps
Chest & Back Straps
Waist Straps
Back D-Ring
Shoulder Adjustment
Legible Label
Shoulder Straps
Chest & Back Straps
Waist Straps
Leg Straps
Cuts
Burns
Holes
Deterioration
Corrosive/ worn out
Color code
Others (Specify)
Project Information
Project Name: Location:
Company name : Date:
Remarks:
Inspector Name: Signature:
Reviewed By HSE Manager / Incharge Signature:
GENERAL SITE SAFETY RULES Form # HSEQ - Rev 2.docx
GENERAL SITE SAFETY RULES Form # HSEQ - Rev 2.docxDwarika Bhushan Sharma
Ã˝
Always wear proper personal protective equipment and inspect and maintain it. You are responsible for your own safety and others, so report any unsafe acts or conditions and avoid taking shortcuts or engaging in horseplay or fights. Communicate risks and follow all safety procedures and instructions.HAZARDOUS SUBSTANCE CHECKLIST Form # HSEQ - HSC Rev 2 -.docx
HAZARDOUS SUBSTANCE CHECKLIST Form # HSEQ - HSC Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name:
Location:
Company Name: Date :
Sl. No Description Yes No N/A Comments
1. Properly stored, labeled, ventilated, isolated, Log and suitable signs displayed.
2. Material Data Safety Sheet (MSDS) available, and communicated to concerned personnel.
3. Adequate/ Sufficient firefighting equipment are in place.
4. Emergency escape and breathing apparatus available, tested and in good condition.
5. Hazardous substances containers/drums have eligible labeling and protected from leakages or spillage.
6. Personnel must be trained in chemical handling.
7. Emergency control plan must be made available, spillage control kits must be available.
8. Empty hazardous substances containers, drums and receptacles should be properly maintained and controlled.
9. Expired chemicals are logged, segregated and disposed properly
10. Others Specify
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
CONCRETE PUMP & EXTENSION PIPELINE Form # HSEQ - CPC Rev 2.docx
CONCRETE PUMP & EXTENSION PIPELINE Form # HSEQ - CPC Rev 2.docxDwarika Bhushan Sharma
Ã˝
Project Information
Project Name: Concrete Pump Reg. No:
Location: Operators Name:
Company Name: Date :
Sr. Description Yes No N/A Comments
1. Concrete Pump 3rd Party Certificate & Registration
2. Sonographic test of all pipes
3. Calibration of all the pressure gauges
4. Operator’s Competency Certificate & Driver’s License
5. Safe distance from the edge of the excavation
6. Outrigger pads are free from damage
7. Outriggers are level
8. Reverse alarm and beacon light are operational
9. Whip arrester on the pipes and pump
10. Safe access for concrete mixer to the area (In/Out)
11. Area properly barricaded and signage posted
12. Hydraulic Oil / Diesel Leakage
13. Extension Pipeline - Free from damage
14. Extension Pipeline -Locking pin in every connection
15. Extension Pipeline - Adequately supported & secured
16. Spillage control measure in place
17. Other accessories e.g. spider pacing boom 3rd party certificate
18. Static pumps positioned properly
19. Static pumps – concrete pipes fixed on structure as per design
20. Concrete pipes coupler pins provided
21. Concrete pipes on floor – away from scaffolds/ formworks
22. Competent banks man and supervision provided
23. Others (Specify)
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
Noted by Project Leader Signature:
BEHAVIORAL OBSERVATION Form # HSEQ BO Rev.0.docx
BEHAVIORAL OBSERVATION Form # HSEQ BO Rev.0.docxDwarika Bhushan Sharma
Ã˝
Project Behavioral Observation Form
Process Observed
Works Package
Subcontractor / CName
Date _ _ /_ _ /_ _ Time from ______ to ______ Duration Mins _____
Checklist attached ‚òê
Video ‚òê
Photo (s) ‚òê
Observation Summary (Ref checklist for details)
Safe ‚òê
Unsafe Acts ‚òê
Safe ‚òê
Unsafe conditions ‚òê
Status:
A. All activities conducted in a safe manner ‚òê
No negative observations
B. Generally conducted in a safe manner ‚òê
Some aspects of the process require improvement
C. Partially conducted in a safe manner ‚òê
One aspect of a task needs improvement
D. Some individual lapses ‚òê
One person working unsafely part of the time
E. Generally conducted in unsafe manner ‚òê
More than one person working unsafely
ATC Engineer-in-charge Supervisor
Follow up Action
‚òê
Analysed by HSE Manager and responsible person _________________
‚òê
Reported / shown to team observed
‚òê
Recommended Action
‚òê
Follow up recommendation
FIRE PREVENTION CHECKLIST Form # HSEQ - FPC Rev 2 -.docx
FIRE PREVENTION CHECKLIST Form # HSEQ - FPC Rev 2 -.docxDwarika Bhushan Sharma
Ã˝
SR. TITLE YES NO N/A Comments
1 FIRE PROTECTION EQUIPMENT
1.1 Are adequate fire-fighting equipment and sufficient extinguishing agents available and operative at all times? ÔÇ£
ÔÇ£
ÔÇ£
1.2 Have workers been oriented on their correct use and operation? ÔÇ£
ÔÇ£
ÔÇ£
1.3 Are portable fire extinguishers of sufficient capacity (at least 20 lbs.) and type available and strategically positioned near hazardous work such that the travel distance to the nearest unit is no greater than 15 meters? ÔÇ£
ÔÇ£
ÔÇ£
1.4 Are regular checks undertaken to make sure that the equipment is not missing or damaged? ÔÇ£
ÔÇ£
ÔÇ£
1.5 Is a fully operational yard hydrant/Fire Hose reel system available prior to start of construction (excluding foundation work) and during the entire construction period?
Where street hydrants are not available, are temporary hydrants provided? ÔÇ£
ÔÇ£
ÔÇ£
1.6 Is a waterline extended as soon as possible behind construction to supplement the Fire Extinguishers placed throughout the construction area? ÔÇ£
ÔÇ£
ÔÇ£
1.7 Are permanent standpipes extended as close as possible behind construction to allow use in case of fire? ÔÇ£
ÔÇ£
ÔÇ£
1.8 Are fully operative standpipes (wet risers) installed up to one level below the highest current work level and are sealed by temporary end caps? ÔÇ£
ÔÇ£
ÔÇ£
1.9 (The following is a less stringent alternative to Item 8 above)
Where construction involves buildings more than 23 meters high, are fully operative standpipes (wet risers) available not less than
3 levels below the highest level under construction.
Where the provision of wet risers does not impede structural work, are they provided to the level below the highest level under construction? ÔÇ£
ÔÇ£
ÔÇ£
1.10 Are the cabinets containing hose reels and portable fire extinguishers inspected at regular intervals but at least twice a week by competent persons? ÔÇ£
ÔÇ£
ÔÇ£
1.11 Are hydrants and standpipes including fire water supply system designed and installed in compliance with UAE Fire and Life safety COP and according to the relevant internationally recognized codes and standards, e.g., NFPA, FM, etc.? ÔÇ£
ÔÇ£
ÔÇ£
1.12 Is the fire water supply at the site available at the required volume and pressure? ÔÇ£
ÔÇ£
ÔÇ£
1.13 Is storage of any material within 3 meters of fire hydrants/Fire Hose reels strictly prohibited? Is access to the outlets unobstructed? ÔÇ£
ÔÇ£
ÔÇ£
2 COMPARTEMENTATION / SEGMENTATION YES NO N/A COMMENTS
2.1 Are fire compartments as required by local regulations installed as soon as possible after the removal of formwork? ÔÇ£
ÔÇ£
ÔÇ£
2.2 Are openings for lift shafts, service ducts and other voids provisionally closed as soon as possible but not later than at the commencement of fit-out work? ÔÇ£
ÔÇ£
ÔÇ£
3 FIRE PREVENTION : HOT WORK MANAGEMENT YES NO N/A COMMENTS
3.1 Is a “permit to work” system being implemented for all parties engaged in “hot work” of any kind such as but not limited to
– grinding, cutting or welding operations,
– use of blow lamps and torches,
– application of hot bitumen
or any other heat-proCOLD WORK PERMIT Form # HSEQ - CWP Rev 2.docx
COLD WORK PERMIT Form # HSEQ - CWP Rev 2.docxDwarika Bhushan Sharma
Ã˝
This cold work permit document is a 2-page form used to request and approve cold work. It lists the job location and description, tools and materials used, potential hazards, precautions needed, and protective equipment. The form requires signatures from the permit requester, acceptor, issuer, and other parties to hand over responsibility between shifts, declare work completion, ensure the site is left safely, and sign off and cancel the permit.Recently uploaded (20)
Sppu engineering artificial intelligence and data science semester 6th Artif...
Sppu engineering artificial intelligence and data science semester 6th Artif...pawaletrupti434
Ã˝
Sppu University Third year AI&DS Artificial Neural Network unit 1TASK-DECOMPOSITION BASED ANOMALY DETECTION OF MASSIVE AND HIGH-VOLATILITY SES...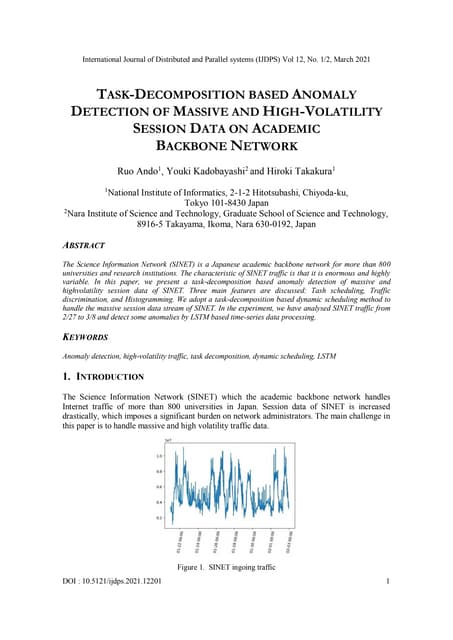
TASK-DECOMPOSITION BASED ANOMALY DETECTION OF MASSIVE AND HIGH-VOLATILITY SES...samueljackson3773
Ã˝
The Science Information Network (SINET) is a Japanese academic backbone network for more than 800
universities and research institutions. The characteristic of SINET traffic is that it is enormous and highly
variable
Design and Analysis of Algorithms Unit 5
Design and Analysis of Algorithms Unit 5sureshkumara29
Ã˝
Algorithm design techniques include:
Brute Force
Greedy Algorithms
Divide-and-Conquer
Dynamic Programming
Reduction / Transform-and-Conquer
Backtracking and Branch-and-Bound
Randomization
Approximation
Recursive Approach
What is an algorithm?
An Algorithm is a procedure to solve a particular problem in a finite number of steps for a finite-sized input.
The algorithms can be classified in various ways. They are:
Implementation Method
Design Method
Design Approaches
Other Classifications
In this article, the different algorithms in each classification method are discussed.
The classification of algorithms is important for several reasons:
Organization: Algorithms can be very complex and by classifying them, it becomes easier to organize, understand, and compare different algorithms.
Problem Solving: Different problems require different algorithms, and by having a classification, it can help identify the best algorithm for a particular problem.
Performance Comparison: By classifying algorithms, it is possible to compare their performance in terms of time and space complexity, making it easier to choose the best algorithm for a particular use case.
Reusability: By classifying algorithms, it becomes easier to re-use existing algorithms for similar problems, thereby reducing development time and improving efficiency.
Research: Classifying algorithms is essential for research and development in computer science, as it helps to identify new algorithms and improve existing ones.
Overall, the classification of algorithms plays a crucial role in computer science and helps to improve the efficiency and effectiveness of solving problems.
Classification by Implementation Method: There are primarily three main categories into which an algorithm can be named in this type of classification. They are:
Recursion or Iteration: A recursive algorithm is an algorithm which calls itself again and again until a base condition is achieved whereas iterative algorithms use loops and/or data structures like stacks, queues to solve any problem. Every recursive solution can be implemented as an iterative solution and vice versa.
Example: The Tower of Hanoi is implemented in a recursive fashion while Stock Span problem is implemented iteratively.
Exact or Approximate: Algorithms that are capable of finding an optimal solution for any problem are known as the exact algorithm. For all those problems, where it is not possible to find the most optimized solution, an approximation algorithm is used. Approximate algorithms are the type of algorithms that find the result as an average outcome of sub outcomes to a problem.
Example: For NP-Hard Problems, approximation algorithms are used. Sorting algorithms are the exact algorithms.
Serial or Parallel or Distributed Algorithms: In serial algorithms, one instruction is executed at a time while parallel algorithms are those in which we divide the problem into subproblems and execute them on different processors. 


Mathematics behind machine learning INT255 INT255__Unit 3__PPT-1.pptx
Mathematics behind machine learning INT255 INT255__Unit 3__PPT-1.pptxppkmurthy2006
Ã˝
Mathematics behind machine learning INT255 
Design of cannal by Kennedy Theory full problem solved
Design of cannal by Kennedy Theory full problem solvedEr. Gurmeet Singh
Ã˝
Design of cannal by Kennedy Theory
By Er Gurmeet Singh
G.C.E.T JAMMU
CONTACT: Gurmeet.b.tech@gmail.com

decarbonization steel industry rev1.pptx
decarbonization steel industry rev1.pptxgonzalezolabarriaped
Ã˝
Webinar Decarbonization steel industryData recovery and Digital evidence controls in digital frensics.pdf
Data recovery and Digital evidence controls in digital frensics.pdfAbhijit Bodhe
Ã˝
This topic contain information about Data recovery and Digital evidence controls in cyber and digital awareness
Biases, our brain and software development
Biases, our brain and software developmentMatias Iacono
Ã˝
Quick presentation about cognitive biases, classic psychological researches and quite new papers that displays how those biases might be impacting software developers.AI ppt on water jug problem by shivam sharma
AI ppt on water jug problem by shivam sharmaShivamSharma588604
Ã˝
this ppt is made on the topic of water jug problem.1-Nature of Software Software Engineering Software process project product Pr...
1-Nature of Software Software Engineering Software process project product Pr...UjjwalAgrawal34
Ã˝
Nature of Software EngineeringSoil Properties and Methods of Determination
Soil Properties and Methods of DeterminationRajani Vyawahare
Ã˝
This PPT covers the index and engineering properties of soil. It includes details on index properties, along with their methods of determination. Various important terms related to soil behavior are explained in detail. The presentation also outlines the experimental procedures for determining soil properties such as water content, specific gravity, plastic limit, and liquid limit, along with the necessary calculations and graph plotting. Additionally, it provides insights to understand the importance of these properties in geotechnical engineering applications.1-HAZARDOUS CHEMICALS.pdf
- 1. Company Name