26. HEMOGLOBINOPATHIES for hematology.pptx
ŌĆóDownload as PPTX, PDFŌĆó
0 likesŌĆó7 views

for HB pathy


















26. HEMOGLOBINOPATHIES for hematology.pptx
- 1. 1 HEMOGLOBINOPATHIES -sickle cell and thalassemia- Wedn,13th . Jan.2021. Presenter: dr. feksi - Resident sem.3 supervisor: dr. lilian- speciacist radiologist.
- 2. 2 OUTLINE ’ü▒Introduction ’ü▒Clinical features ’ü▒Imaging features ’ü▒Differential diagnosis ’ü▒References.
- 3. 3 INTRODUCTION ’ü▒Inherited, autosomal recessive genetic conditions. ’ü▒Sickle cell ( Qualitative Defect), Thalassaemia (Quantitative Defect). ’ü▒Sickle cell condition results from a single amino acid substitution ( valine for glutamic acid) at position 6 of B-globin gene. Forms: Hemoglobin(Hb F, A, S, C, thal) ’ü▒Thalassaemia ŌĆōIneffective erythropoiesis results to reduced erythroblast maturation and early death of red cell precursors. a-thalassaemia and b-thalassaemia
- 4. 4 INTROŌĆ”.epidemiology. ’ü▒No gender predilection. ’ü▒Sickle cell condition highest in Africa, Middle East and Mediterranean countries. In black Americans reported to occur 3cases in every 1000 live births. ’ü▒B-thalassemia highest in Mediterranean, parts of Africa and Asia. a-thalassemia highest amongst people from Asia. ’ü▒They contribute to mortality and morbidity and life span ranges 30 to 45 years.
- 5. 5 CLINICAL PRESENTATIONS. ’ü▒Anemia* ’ü▒Vaso-oclussive crises ’āśMuscle/Bone pain* ’āśBrain-stroke, cognitive impairment. ’āśPulmonary-Acute chest syndrome, Recurrent pneumonia/Chronic lung diseases (impaired immunity due to functional asplenia) ’āśAbdomen- abdominal pain, sequestration syndrome. ’ü▒Others. ’āś Impaired immunity from autosplenectomy ’āś Leg ulcers ’āś Priapism ’āś Renal failure ’āś Ocular and orbital complications.
- 7. 7 IMAGING FEATURES. ’ü▒Marrow hyperplasia. ’āśSKULL-Cortical thinning,Osteopenia,Hair on End sign, Thinning of outer table skull , widening diploic space. SPINE-H-Shaped VB, Fish mouth sign, Vertebral collapse with resultant kyphosis. LONG BONES-widening medullary space, ’āśObliteration of paranasal sinuses ’āśMaxillary alteration( hypertelorism, malocclusion of jaws) ’āśDisplacement of dental structures ( Rodent facies) ’āśErlenmeyer flask deformity( in long tubular bones) ’ü▒Growth defect/Premature fusion of growth plate. ’ü▒Osteosclerosis ’ü▒Osteonecrosis. ’ü▒Infection:Dactylitis,Periostitis,Osteomylitis. ’ü▒Fructure secondary to osteoporosis/Infection.
- 8. 8 Marrow hyperplasia. Normal scan Hair on end
- 9. 9 Marrow hyperplasia. Normal scan Fish Mouth & H- Vertebrae
- 10. 10 Marrow hyperplasia Normal scan Widening medullary space
- 11. 11 Growth defect Normal scan. Epiphyseal/carpal deformity.
- 12. 12 Dactylitis Physical examination Hand foot syndrome
- 14. 14 Acute osteomyelitis/Infarction Acute bone infarction. Axial T2-weighted MR images of the femur in a 13-year-old boy with leg pain. RIGHT: Initial image shows regions of both high and low signal intensity within the medullary cavity and high signal intensity in the vastus intermedius muscle, features that may represent either infarction or infection. Infection was not suspected clinically. LEFT: Follow-up image obtained after 4 weeks of standard management shows resolution of the area of low signal intensity within the medullary cavity and the area of high signal intensity in the adjacent muscle, a finding indicative of infarction.
- 15. 15 Infarction ’ü▒Infarction in a 12-year-old boy with homozygous sickle cell disease, left tibial pain, and a lowgrade fever. Medial (left) and lateral (right) views of the left (L) tibia from late static phase 99mTc MDP scintigraphy show an area of decreased tracer uptake within the proximal shaft (arrowheads), a finding suggestive of infarction ’ü▒Anterior views of both tibiae (a) and bothankles (b) from 99mTc hexamethylpropyleneamine oximeŌĆōlabeled leukocyte imaging .The appearance of increased radiotracer uptake localized to the region of the left (L) ankle (arrowhead in b) supports a diagnosis of infection. The incidentally observed absence of activity in the upper shaft of the left tibia (arrow in a) is indicative of bone infarction.
- 16. 16 Differential diagnosis: Myelofibrosis ’ü▒Coronal CT of the chest demonstrating extra medullary hematopoiesis in the posterior mediastinum, which typically appear as bilateral and symmetrical posterior mediastinal masses (white arrows) ’ü▒Extra medullary hematopoiesis. T2-weighted coronal (a) and sagittal (b) MR images of the thoracolumbar spine in a 47-year-old woman show a right-sided paravertebral soft-tissue mass (arrow). The mass had intermediate signal intensity on both T1- and T2-weighted images, similar to the signal intensity of normal intramedullary hematopoietic tissue. Vertebral endplate depression due to central infarction also is depicted.
- 17. 17 Differential diagnosis: Multiple Myeloma
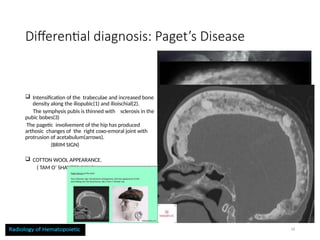
- 18. 18 Differential diagnosis: PagetŌĆÖs Disease ’ü▒ Intensification of the trabeculae and increased bone density along the iliopubic(1) and ilioischial(2). The symphysis pubis is thinned with sclerosis in the pubic bobes(3) The pagetic involvement of the hip has produced arthosic changes of the right coxo-emoral joint with protrusion of acetabulum(arrows). (BRIM SIGN) ’ü▒ COTTON WOOL APPEARANCE. ( TAM OŌĆÖ SHANTER SIGN)
- 19. 19 Summary. ’ü▒Bone abnormalities in SCA result secondary to marrow hyperplasia and episodes of ischemia leading to infarction ’ü▒Clinical presentations have a great role in excluding differential diagnosis. ’ü▒Multiple modalities can be used in conjunction with one another to image these bony changes.
- 20. 20 References. ’ü▒Radiopedia ’ü▒Musculoskeletal Manifestations of Sickle Cell Disease, Vivian C. Ejindu, MRCP, Andrew L. Hine, FRCR, Mohammad Mashayekhi, FRCR, Philip J. Shorvon, FRCR, and Rakesh R. Misra, FRCR ’ü▒Principles of diagnostic radiology, William E Brant, 4th edition ’ü▒Radiologic Manifestations of Bone Disease in Sickle Cell Anemia. Oni J. Blackstock, HMS III, Gillian Lieberman, MD
Editor's Notes
- #1: Sickle cell and thalassaemia are the common hemoglobinopathies that result to MSK pathologies. Medical imaging modalities can play part as a primary diagnostic modality in MSK.
- #2: They share similar presentations.
- #3: Sickle cell condition results from either homozygous(HB SS) or heterozygous( when it combines with other abnormal Hb, like HB SC or S-THAL) The combination of a sickle B Globin gene with a normal one ( HB SA) results in a sickle cell trait, with no resultant complication. Thalassemia described according to severity; Thalassaemia minor, intermediate and major( a cause of hydrops fetalis). Thalassemia trait more common cause s insignificant complications, protects against malaria.
- #5: 1.Deoxygenation of HB SŌĆōcontaining red blood cells results in the aggregation of abnormal hemoglobin molecules into long chains. this irreversible process distorts the red blood cell into a rigid sickle shape, the consequences are obstruction of the microcirculation, ischemia, and infarction. 2.Anemia results from the rapid removal of abnormal red blood cells by the reticuloendothelial system, which reduces the red cell life span to one-tenth its normal duration. 3.The earliest manifestation is usually in early childhood, as babies are protected by elevated levels of fetal haemoglobin (hbf) in the first 6 months . 4.The first presentation is commonly with a painful vaso-occlusive crisis (sudden onset of bone or visceral pain due to micro-vascular occlusion and ischaemia, often in the setting of sepsis or dehydration.)
- #6: 1. CT-best technique in assessment of matrix mineralization, cortical detail, and detection of the cystic and fatty lesions. -Can identify subtle bony abnormalities (occult fractures) and their relationship to adjacent organs Weakness-May fail to demonstrate early vascular and marrow abnormality. 2.MRI-Sensitive to changes in bone marrow (i.e. subtle marrow edema, marrow infarcts) -Can detect and stage primary bone tumors and occult bony metastases. Weakness-Difficulty visualizing fine bone detail or small calcifications. 3.Bone scanogragm/ scientigraph:This modality also plays a role in detecting osteomyelitis. Likewise, indium leukocyte scanning has an important role in diagnosing osteomyelitis.
- #7: SPINE-Cortical thinning and softening of bone produce a smooth biconcave deformity of the vertebral bodies -adjacent intervertebral disks compress the endplates, giving the vertebrae the characteristic ŌĆ£fish-mouthŌĆØ appearance.
- #11: Marked carpal deformities in the left wrist in a young woman. Radiograph shows the fusion of several intercarpal joints, a condition that affected the patientŌĆÖs grip. Growth disturbance in the distal radius in a 12- year-old girl. Anteroposterior radiograph of the left wrist shows epiphyseal shortening and a cup deformity of the adjacent metaphysis.
- #12: Dactylitis in the feet of a 1-year-old child. Radiograph shows periosteal new bone formation along the shafts of the metatarsals in the right foot (arrows) and marked destructive changes that may lead to permanent deformity of the fourth metatarsal in the left foot. Dactylitis ( hand foot syndrome) is an early manifestation of scd in first two years of life which results from bone infarcts in the diaphyses of small long bones; Imaging findings include: Patchy areas of lucency ,periostitis .Soft tissue swelling of metacarpals or metatarsals which could be difficult to distinguish from osteomyelitis
- #16: Myelofibrosis is a chronic stem cell disorder that results in a build up of marrow fibrosis and dysfunction, hypermetabolic states and myeloid metaplasia. Shows clinical and radiological manifestation of osteosclerosis and extra medullary haematopoiesis to thrombohaemorrhagic complication from haemostatic dysfunction.
- #17: Radiograph showing multiple very sharply outlined (punched out) lytic lesions of multiple myeloma (DEFECT IN SKULL). Collection of plasma cell in the bone that eat up the bone and make it looks like dots appearing Multiple myeloma is a cancer of plasma cells that produce monoclonal immunoglobulin and invade and destroy adjacent bone tissue. Common manifestations include lytic lesions in bones causing pain, and/or fractures, renal insufficiency, hypercalcemia, anemia, and recurrent infections.
- #18: Paget disease┬Āof the bone┬Āis a common,┬Āchronic bone disorder characterized by excessive abnormal bone remodeling. The classically described radiological appearances are expanded bone with a coarsened trabecular pattern. The pelvis, spine, skull, and proximal long bones are most frequently affected Paget disease┬Āof the bone┬Āis a common,┬Āchronic bone disorder characterized by excessive abnormal bone remodeling. The classically described radiological appearances are expanded bone with a coarsened trabecular pattern. The pelvis, spine, skull, and proximal long bones are most frequently affected. SKULL: O steoporosis circumscrepta, Cottonwool appearance, Diploic widening, Tam OŌĆÖ Shanters sign. SPINE: Picture frame sign, Vertebral square, Vertical tribecular thickening. PELVIS: Brim sign, Acetabular protrusion, enlargement of pubic rami and ischium. LONG BONE: Blade of glass or candle frame sign.
- #20: THANK YOU!