8. neuro monitoring during ecmo #beach2019 (taccone)
ŌĆóDownload as PPTX, PDFŌĆó
2 likesŌĆó282 views

This workshop will outline the basic principles of extracorporeal life support made easy by key-experts in the field. During the course delegates will gain a good understanding of ECMO in the following areas: Theoretical concepts, basic physiology and pathophysiology, cardiac and respiratory support and monitoring, alarm settings and monitoring, role of cardiac ultrasound during ECMO, newest technologies, circuits and devices, practical hands-on sessions and simulations.






















![BEACH 2019 ŌĆō FS Taccone
T1T2T3T4T5T6
T7T8
T9
T10
T11T12L1L2L3
Higher R/LD: 12 [6-13]% vs. 5 [4-7]% - p=0.005
(1 patient with posterior stroke had R/LD < 10%)
CVA = 10 patients (18% - 9 isch / 1 hh)
8 hours before pupillary dilatation
RIGHT
LEFT
CEREBRAL OXYGEN SATURATION](https://image.slidesharecdn.com/8-191013121645/85/8-neuro-monitoring-during-ecmo-beach2019-taccone-28-320.jpg)
![BEACH 2019 ŌĆō FS Taccone
T1T2T3T4T5T6
T7T8
T9
T10
T11T12L1L2L3
Cerebral Desaturation = 43 patients (77%)
Desaturation
(n=43)
Non-desaturation
(n=13)
Age, years 58 [46-63] 53 [40-60]
Male gender, n (%) 29 (67) 11 (84)
SOFA on ECMO 12 [11-15] 9 [8-11] *
Acute CNS failure, n (%) 22 (51) 1 (8) *
Bleeding, n (%) 29 (67) 7 (54)
Lactate on ECMO, n (%) 4.2 [2.7-8.5] 3.5 [3.0-6.6]
Seizures, n (%) 2 (5) -
Stroke, n (%) 10 (23) -
Brain death, n (%) 9 (21) -
Hospital mortality, n (%) 32 (74) 4 (36) *
CEREBRAL OXYGEN SATURATION](https://image.slidesharecdn.com/8-191013121645/85/8-neuro-monitoring-during-ecmo-beach2019-taccone-29-320.jpg)












8. neuro monitoring during ecmo #beach2019 (taccone)
- 1. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 BEACH 2019 ŌĆō FS Taccone Neurological Monitoring during ECMO Fabio Silvio TACCONE, MD, PhD Dpt of Intensive Care Brussels, Belgium
- 2. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3
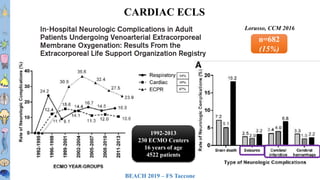
- 3. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 CARDIAC ECLS Lorusso, CCM 2016 n=682 (15%) 14% 19% 67% 1992-2013 230 ECMO Centers 16 years of age 4522 patients
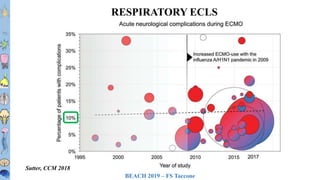
- 4. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 Sutter, CCM 2018 RESPIRATORY ECLS
- 5. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 Lorusso, CCM 2016 89% vs. 53% ECLS AND NEUROLOGICAL COMPLICATIONS
- 6. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3
- 7. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 HOW TO DETECT ?
- 8. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 CLINICAL EXAMINATION ŌĆ” remains the best ┬½ tool ┬╗ to evaluate the functional status, the severity of injury and assess prognosis in brain diseases
- 9. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 SEDATION ANOXIC INJURY ENCEPHALOPATHY CLINICAL EXAMINATION AND ECLS
- 10. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 ’ā╝Pre-ECMO characteristics ’ā╝Hypoxemia ’ā╝CVA ’ā╝Age ’ā╝Infection with neurological involvement (H1N1 ŌĆō HIV?) ’ā╝Pre-ECMO Cardiac arrest ’ā╝On sedation / NMBAs ’ā╝Duration of MV - RRT ’ā╝Coagulation disorders ŌĆō Use of anticoagulation WHO SHOULD WE MONITOR ?
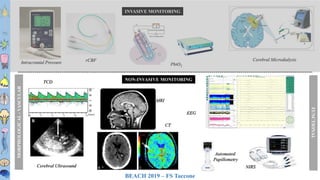
- 11. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 INVASIVE MONITORING NON-INVASIVE MONITORING PbtO2 Cerebral Microdialysis TCD NIRS rCBFIntracranial Pressure EEG FUNCTIONAL Cerebral Ultrasound MRI CT MORPHOLOGICAL-VASCULAR Automated Pupillometry
- 12. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 BRAIN IMAGING ’ā╝ 30-50% of CT findings that would affect therapy (and prognosis) ’ā╝ More frequent in older patients and in patients with long ECMO runs ’ā╝ More frequent in delayed clinical improvement
- 13. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 BRAIN IMAGING
- 14. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 39 STUDIES ŌĆó Neonates (n=30) ’ā╝ Head US (n=12) ŌĆó Retrospective (n=17) ŌĆó No Interventional Low to very-low QOE Small size Heterogeneous and selected populations WHICH NEUROMONITORING ?
- 15. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 BRAIN ULTRASOUND
- 16. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 Lateral Ventricles Third Ventricle Brainstem
- 17. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 BRAIN ULTRASOUND
- 18. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 ŌĆó Clinics ŌĆó ECG ŌĆó Echocardio ŌĆó Troponin ŌĆó SvO2 + Lactate ŌĆó Clinics ŌĆó EEG ŌĆó TCD ŌĆó NSE/S100B ŌĆó BrainOx WHICH NEUROMONITORING ?
- 19. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 CEREBRAL OXYGEN SATURATION DO2 MAP / CO CO2 / ICP Diffusion/ Microcirculation VO2 Seizures / t┬░
- 20. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 CEREBRAL OXYGEN SATURATION
- 21. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 rSO2(%) CEREBRAL OXYGEN SATURATION
- 22. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 MAP 65 mmHg ECMO 3.5 L/min
- 23. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 MAP 78 mmHg ECMO 4.0 L/min
- 24. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 VA-ECMO CEREBRAL OXYGEN SATURATION
- 25. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 VA-ECMO VV-ECMO CEREBRAL OXYGEN SATURATION
- 26. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 CEREBRAL OXYGEN SATURATION
- 27. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 ’ā╝ Retrospective analysis ’ā╝ 159 patients on V-A ECMO ’ā╝ November 2008 to December 2015 ’ā╝ Concomitant rSO2 monitoring ’ā╝Baseline mean rSO2 ’ā╝Percentage of time mean rSO2 was under 60% (e.g. > 5% of the monitoring period) = CEREBRAL DESATURATION ’ā╝Maximum differential in right/left (R/LD) StcO2 ’ā╝Correlation between mean rSO2 and R/LD and clinical events (stroke, differential hypoxia, survival) Pozzebon, Neurocrit Care 2018 56 (35%) with rSO2 monitoring CEREBRAL OXYGEN SATURATION
- 28. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 Higher R/LD: 12 [6-13]% vs. 5 [4-7]% - p=0.005 (1 patient with posterior stroke had R/LD < 10%) CVA = 10 patients (18% - 9 isch / 1 hh) 8 hours before pupillary dilatation RIGHT LEFT CEREBRAL OXYGEN SATURATION
- 29. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 Cerebral Desaturation = 43 patients (77%) Desaturation (n=43) Non-desaturation (n=13) Age, years 58 [46-63] 53 [40-60] Male gender, n (%) 29 (67) 11 (84) SOFA on ECMO 12 [11-15] 9 [8-11] * Acute CNS failure, n (%) 22 (51) 1 (8) * Bleeding, n (%) 29 (67) 7 (54) Lactate on ECMO, n (%) 4.2 [2.7-8.5] 3.5 [3.0-6.6] Seizures, n (%) 2 (5) - Stroke, n (%) 10 (23) - Brain death, n (%) 9 (21) - Hospital mortality, n (%) 32 (74) 4 (36) * CEREBRAL OXYGEN SATURATION
- 30. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 CEREBRAL OXYGEN SATURATION
- 31. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 n=26 (62% were normal ŌĆō 3/26 (11%) had seizures) n=20 (no changes in background during ECMO ŌĆō no lateralization) ELECTROENCEPHALOGRAPHY (EEG)
- 32. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 Time to first seizure At least 24h; 48h if coma or lateralized periodic discharges Percentageofpatients ELECTROENCEPHALOGRAPHY (EEG)
- 33. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 Sinnah, CCM 2018 n=22 cEEG VA-ECMO Poor Outcome 50% ELECTROENCEPHALOGRAPHY (EEG)
- 34. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 ELECTROENCEPHALOGRAPHY (EEG) EEG FEATURES ALL N=139 V-A ECMO N=98 V-V ECMO N=41 ANY ANOMALIES 86 (62) 65 (66) 21 (51) SEIZURES 16 (12) 8 (8) 8 (20) GPDs/LPDs 9 (6) 6 (6) 3 (7) SEVERE ENCEPHALOPATHY 36 (26) 30 (31) 6 (14) FLAT/BS 31 (22) 23 (24) 8 (20) ASYMMETRY 26 (19) 19 (19) 7 (17) UNREACTIVE 67 (48) 53 (54)* 14 (34)*Unpublished Data
- 35. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 BRAIN BIOMARKERS Zetterberg, Nature Review Neurol 2013
- 36. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 n=15 (VA in 10) 3 had brain complications * BRAIN BIOMARKERS
- 37. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 AUC Ōēł 0.70 / Cut-offs ??? n=80 (2010-2013) ŌĆō 41% unfavorable outcome and 31% CT abnormalities BRAIN BIOMARKERS
- 38. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 rSO2 (c)EEG CT-scan Biomarkers ?? LETŌĆÖS PUT ALL TOGETHER !!!
- 39. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 VV-ECMO VA-ECMO ECPR ’ā╝X ’ā╝X ’ā╝X ’ā╝X ’ā╝X ’ā╝X ’ā╝X ’ā╝X ’ā╝X LETŌĆÖS PUT ALL TOGETHER !!! ’ā╝X
- 40. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3 n = 16 n = 19 n = 18 n = 27 ’ā╝ Neurological complications during ECMO are frequent ’ā╝ Neuro-monitoring may help in detecting brain ŌĆ£dysfunctionŌĆØ (perfusion, oxygenation or seizures) ’ā╝ rSO2 and (c)EEG ’ā╝ May help with prognosis CONCLUSIONS
- 41. BEACH 2019 ŌĆō FS Taccone T1T2T3T4T5T6 T7T8 T9 T10 T11T12L1L2L3
Editor's Notes
- #5: Renal Failure CrCL + thromobocytopenia (LONDON) Pre-arrest ŌĆō High BIL and CRRT (ELSO) ŌĆō Mortality 75% , different ICH>stroke>seizures
- #6: 7% in the ELSO registry ŌĆō half ICH
- #7: Embolic events Anticoagulation Previous brain injury and BBB disruption Carotid cannulation Venous congestion Non-pulsatile flow
- #11: Embolic events Anticoagulation Previous brain injury and BBB disruption Carotid cannulation Venous congestion Non-pulsatile flow
- #20: Near infrared spectroscopy is a non invasive technique which employes the use of near infrared wavelenghts emitted by sensor pads to evaluate regional oxygenation of the organ or tissue monitored. The difference in absorption of these wavelenghts by oxygenated and deoxigenated Hb is calculated,providing the clinician with information regarding the regional oxygen saturation (or saturation of cerebral tissue StcO2. NIRS monitoring is currently used during cardiac surgery, where it has also demostrated to be of great utility and where protocols of neuroprotection NIRS based have also been proposed, but there are only a few datas regarding its use during ECMO in adult population. ThatŌĆÖs why we decided to analyse the datas we collected on patients on NIRS during ECMO.
- #21: In our study we retrospectively analysed our ECMO register and identified n, 159 patients put on VA ECMO from November 2008 to December 2015. 39 were monitored with NIRS.The reasons why these patients were put on ecmo were: cardiogenic shock 19 pzt, ECPR 14 pts and post heart lung Tx 6 pts. X pts had a femoro femoral cannulation, while xŌĆ” pts hada central ECMO: The median age was 54 years, median ECMO duration was 6 days ad median NIRS monitoring was 3 days.
- #22: Wong, Artificial Organs 2012
- #25: Wong, Artificial Organs 2012
- #26: Wong, Artificial Organs 2012
- #27: Wong, Artificial Organs 2012
- #28: In our study we retrospectively analysed our ECMO register and identified n, 159 patients put on VA ECMO from November 2008 to December 2015. 39 were monitored with NIRS.The reasons why these patients were put on ecmo were: cardiogenic shock 19 pzt, ECPR 14 pts and post heart lung Tx 6 pts. X pts had a femoro femoral cannulation, while xŌĆ” pts hada central ECMO: The median age was 54 years, median ECMO duration was 6 days ad median NIRS monitoring was 3 days.
- #29: In our study we retrospectively analysed our ECMO register and identified n, 159 patients put on VA ECMO from November 2008 to December 2015. 39 were monitored with NIRS.The reasons why these patients were put on ecmo were: cardiogenic shock 19 pzt, ECPR 14 pts and post heart lung Tx 6 pts. X pts had a femoro femoral cannulation, while xŌĆ” pts hada central ECMO: The median age was 54 years, median ECMO duration was 6 days ad median NIRS monitoring was 3 days.
- #30: In our study we retrospectively analysed our ECMO register and identified n, 159 patients put on VA ECMO from November 2008 to December 2015. 39 were monitored with NIRS.The reasons why these patients were put on ecmo were: cardiogenic shock 19 pzt, ECPR 14 pts and post heart lung Tx 6 pts. X pts had a femoro femoral cannulation, while xŌĆ” pts hada central ECMO: The median age was 54 years, median ECMO duration was 6 days ad median NIRS monitoring was 3 days.
- #31: In our study we retrospectively analysed our ECMO register and identified n, 159 patients put on VA ECMO from November 2008 to December 2015. 39 were monitored with NIRS.The reasons why these patients were put on ecmo were: cardiogenic shock 19 pzt, ECPR 14 pts and post heart lung Tx 6 pts. X pts had a femoro femoral cannulation, while xŌĆ” pts hada central ECMO: The median age was 54 years, median ECMO duration was 6 days ad median NIRS monitoring was 3 days.
- #33: STROKE ŌĆō localization; extention ICH ŌĆō localization; hematoma volume SAH ŌĆō extension of hemorrhage (Fisher scale)
- #34: STROKE ŌĆō localization; extention ICH ŌĆō localization; hematoma volume SAH ŌĆō extension of hemorrhage (Fisher scale)
- #35: STROKE ŌĆō localization; extention ICH ŌĆō localization; hematoma volume SAH ŌĆō extension of hemorrhage (Fisher scale)
- #36: STROKE ŌĆō localization; extention ICH ŌĆō localization; hematoma volume SAH ŌĆō extension of hemorrhage (Fisher scale)
- #37: May increase before ICH is visible - pediatrics
- #38: STROKE ŌĆō localization; extention ICH ŌĆō localization; hematoma volume SAH ŌĆō extension of hemorrhage (Fisher scale)
- #39: STROKE ŌĆō localization; extention ICH ŌĆō localization; hematoma volume SAH ŌĆō extension of hemorrhage (Fisher scale)
- #40: STROKE ŌĆō localization; extention ICH ŌĆō localization; hematoma volume SAH ŌĆō extension of hemorrhage (Fisher scale)