Pre And Postoperative Care Of The Modern Cataract Patient
ŌĆó
11 likesŌĆó10,928 views

Powerpoint presentation on new technology featuring capsular tension rings, toric IOLs, crystalens and the ReStor IOL.




































Pre And Postoperative Care Of The Modern Cataract Patient
- 1. Pre and Postoperative Care of the Modern Cataract Patient Dean Dornic, MD Laser Eye Center of Carolina
- 2. Disclosures 1. Dinner this evening was provided by Alcon, manufacturers of the Toric and Restor IOLs discussed 2. I am not an investigator or paid consultant for any of the devices or instruments discussed. I have no financial interest in the products or companies discussed
- 3. Disclosures 3. I am a nerd.
- 4. History of Intraocular Lenses A brilliant eye surgeon performs a revolutionary operation in secret, implanting a new device, the intraocular lens, which replaces the cloudy cataract. Word leaks out two years later, and the worldŌĆÖs most prominent ophthalmologist vilifies and ostracizes him. He suffers from depression, an outcast in his profession. He and a handful of other doctors around the world toil in obscurity for three decades, performing a few hundred, and later, a few thousand surgeries a year, advancing the science.
- 5. Vindication Ralph Nader and Sydney Wolfe petition the FDA to outlaw the lens. Robert Young (who played Marcus Welby, M.D. on television), testifies in Washington D.C. that the lens ŌĆ£saved my career and should be available to all Americans.ŌĆØ The lens gains acceptance. 100 million patients around the globe regain their vision from the lens. The surgeon, at 93 years of age, is knighted by Queen Elizabeth.
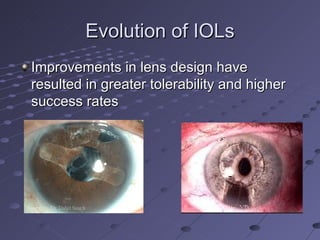
- 6. Evolution of IOLs Improvements in lens design have resulted in greater tolerability and higher success rates
- 7. Better Refractive Outcomes Improvements in instruments, techniques and IOL formulas have led to greater predictability. Immersion ultrasound IOL Master SRK/T, Haigis and Holladay IOL formulas
- 10. Potential Problems in Accurately Picking an IOL Accuracy in measurements Corneal measurements/power Each diopter error in K reading will result in a similar error in final refraction Different densities of cataract Indention of Globe/IOP effect axial length Staphylomas or measurement on optic disc Patient Cooperation A 1 mm error in axial lengthresults in a 3 diopter IOL error
- 11. Potential Problems in Accurately Picking an IOL Problems in Calculations Some formulas do better for very short eyes Some formulas do better for very long eyes There is an assumed position of the IOL Available formulas break down after refractive surgery History is helpful Gas permeable contact lens refraction can help Instruments that measure the central corneal power can be utilized
- 12. Important Points Do not guarantee or imply results Counsel patients on steps that can be done to remedy the situation Prior Refractive Surgery Patients Deserve Extra Attention
- 13. Choosing A Refractive Target Correct both eyes for distance Correct both eyes for near Monovision Correct Astigmatism Correct Presbyopia Accomodating (Crystalens) Multifocal (ReStor or ReZoom)
- 14. How to Choose Ask Listen Be familiar with the nuances of each lens and counsel accordingly Advise of how problems may be ameliorated Underpromise- Do not promise spectacle independence Make a recommendation
- 15. The Accomodating IOL Crystalens 5.0 mm optic Hinged plate with long flexible haptics Relies on forward movement of vitreous Provides about 1.5 D of near add
- 16. Important Considerations Small optic The theoretic amount of accomodation is small based on lens movement The amount of accomodation is dependent on lens power Role of capsular bag size/fibrosis Some training may be necessary
- 17. Bottom Line on Crystalens It performs better than a monofocal IOL for near tasks Probably gives about 1.5 D of functional accomodation for most patients The jury is out on the effect of YAG capsulotomies/capsular bag fibrosis Only about 25% of patients are truly spectacle free if both eyes set for distance
- 18. The Array and ReZoom Refractive multifocal lenses The Array is silicone and now defunct The ReZoom lens is a modification in lens design with larger distance and smaller near zones. Also better blend zones.
- 19. Side Effects of Multifocals By definition, the IOL has at least two focal points and therefore there is a division of light energy Leads to loss of contrast and halos
- 20. What is the AcrySof ® ReSTOR ® IOL? The AcrySof ® ReSTOR ® IOL incorporates an apodized diffractive optic with refraction to achieve a range of quality vision.
- 21. Anatomy of the Apodized Diffractive IOL Step heights decrease peripherally from 1.3 ŌĆō 0.2 microns A +4.0 add at lens plane equaling +3.2 at spectacle plane Central 3.6 mm diffractive structure
- 22. Theoretical Total Energy Balance at 550 nm for AcrySof ® ReSTOR ® Apodized Diffractive Optic Smaller steps further out direct less light to near Grossly magnified schematic . Larger steps at lens center divide light equally between two images 0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1 1 2 3 4 5 6 Pupil Diameter (mm) @ 550 nm Relative Energy Distance Focus Near Focus
- 23. AcrySof® ReSTOR® IOL FDA Clinical Study Results
- 24. Strengths of the AcrySof ® ReSTOR ® IOL High quality uncorrected near and distance vision with 20/40 or better intermediate vision without movement of the IOL 80% Overall Spectacle Freedom Nearly 94% of patients would have the lens again
- 25. Binocular Defocus Curve - A Full Range of Vision ®
- 26. If you understood all graphs
- 27. Visual Disturbances 120-180 Days Post-Operative Night Vision Problems Halos Glare AcrySof ® ReSTOR ® IOL N=457 Monofocal Control N=156 None/Mild Moderate Severe
- 28. Summary of AcrySof ® ReSTOR ® IOL Data indicates the AcrySof ® ReSTOR ® IOL: Provides excellent near VA without compromising distance VA Distance VA (mean uncorrected of 20/20) Near VA (mean uncorrected of 20/25=J1) Increased Spectacle Freedom (80% of patients do not require glasses for daily activities) Provides High Patient Satisfaction (Nearly 94% would have the lens again)
- 30. Available Powers Model Cylinder Power SN6AT3 1.03 D SN6AT4 1.55 D SN6AT5 2.06 D
- 31. Patient Selection The pre-op assessment for the AcrySof toric IOL has two fundamental parts: Keratometry First, the amount of corneal astigmatism that needs to be corrected must be determined. Topography Second, we need to confirm that the astigmatism is regular and for this purpose a topographer is essential.
- 32. Who should be offered a Toric IOL Remember that the important thing is the amount of Corneal astigmatism Lenticular astigmatism is usually ATR The incision may contribute to astigmatism (generally 0.50 D WTR) Even reduction of astigmatism is generally appreciated
- 33. Keys to Success with Presbyopia Correcting IOLs Undersell. Do not promise spectacle independence. Remind patients that full benefits will not be realized until both eyes are implanted Ask if they do a lot of night driving. Ask about midrange tasks (computer etc.) Consider a questionaire Warn them that they may require ŌĆśTouch-upsŌĆØ Accurate measurements and modern lens calculation formulas are key
- 34. Keys to Success Extra testing may be necessary Topography OCT Careful Preop examination Corneal dystrophies Dry Eyes PXF Retinal disorders
- 35. Which Cataract Patients Should Be Offered A Multifocal IOL? All patients without a monovision IOL in the fellow eye Beware of pre-existing pathology Warn about night halos Medicare and Private Insurance will not cover the cost associated with these IOLs Do not assume that these IOLs are cost prohibitive
- 36. Patient Selection Pre-operative Considerations Considerations Patients who no longer desire to wear glasses Functional and occupational requirements Ocular pathology Patients visual demands Expectation for near vision needs
- 37. Patient Selection Pre-operative Exclusion Criteria Subjective Exclusion Hypercritical patients Patients with unrealistic expectations Medical Exclusion Pre-existing ocular pathology Previous refractive patients? Individuals with a monofocal lens
- 38. Trouble Shooting Correction of residual refractive error can be crucial Remind Crystalens patients that accomodation must be built up Remind patients of set bifocal distance (13 inches) Demonstrate with -3 trial lens what their near vision would be like without the bifocal
- 39. Trouble Shooting Look for concomitant pathology Treat dry eye aggressively Earlier YAG lasers Treat/prevent CME Remind of need for patience Improved accomodation Reduction in halo Need for neuroadaptation
- 41. ╠²
- 42. ╠²
- 43. Thank You