

Absorb user forum bvs in bifurcation dr vsp
- 1. Clinical History: ’ü¼55 Yrs Male. ’ü¼DM ’ü¼Previous CAG 2009, Class II Angina ’ü¼TMT Positive for inducible ischaemia ’ü¼Normal LV Function by 2D Echo
- 2. CAG ŌŚÅ CAG at Right Radial Approach ŌŚÅ LAD after D1 50% lesion, Proximal Calcium. ŌŚÅ D1 - Medina : 0,0,1 , Tight Stenoses with Calcium.
- 3. Strategy: ’ü¼ Deploy Absorb - BVS after POBA to D1
- 4. PCI Hardware: ŌĆó Rt Radial approach -6F Teurmo sheath, Guiding: EBU 3.5-6F, ŌĆó Guide wire: -BMW ŌĆō to D1. ŌĆó QCA: D1 80% stenosis, Diameter: 2.5mm, length: 15mm.
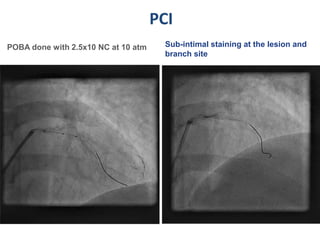
- 5. PCI POBA done with 2.5x10 NC at 10 atm Sub-intimal staining at the lesion and branch site
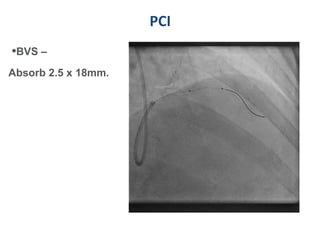
- 6. PCI ŌĆóBVS ŌĆō Absorb 2.5 x 18mm.
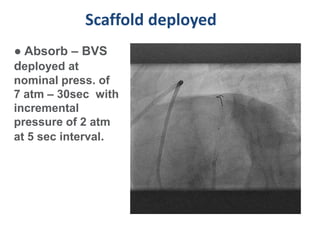
- 7. Scaffold deployed ŌŚÅ Absorb ŌĆō BVS deployed at nominal press. of 7 atm ŌĆō 30sec with incremental pressure of 2 atm at 5 sec interval.
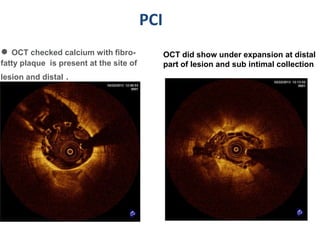
- 8. PCI ŌŚÅ OCT checked calcium with fibro- OCT did show under expansion at distal fatty plaque is present at the site of part of lesion and sub intimal collection lesion and distal .
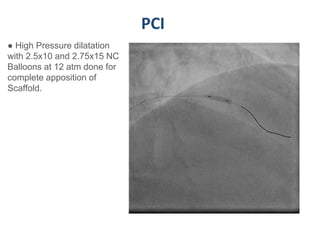
- 9. PCI ŌŚÅ High Pressure dilatation with 2.5x10 and 2.75x15 NC Balloons at 12 atm done for complete apposition of Scaffold.
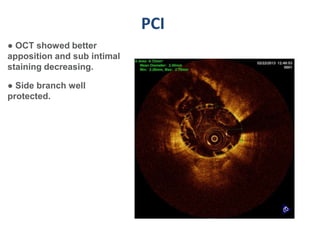
- 10. PCI ŌŚÅ OCT showed better apposition and sub intimal staining decreasing. ŌŚÅ Side branch well protected.
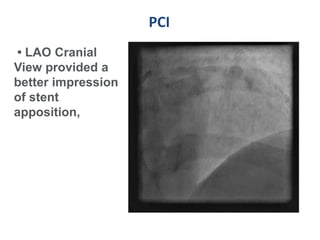
- 11. PCI ŌĆó LAO Cranial View provided a better impression of stent apposition,
- 12. Message ’ü¼ BVS Absorb needs proper bed preparation with NC Balloon for calcific lesions. ’ü¼ High Pressure Dilatation with sub Intimal Collection can lead to vessel damage and perforation. ’ü¼ OCT guidance is obligatory for Absorb BVS.
- 13. THANK YOU