Acj excision watanabe india

This document discusses the anatomy and surgical procedure of AC joint excision. It begins by describing the anatomy of the AC joint, including the fibrocartilage discs and ligaments. It then discusses the indications for AC joint excision as symptomatic osteoarthritis or painful osteolysis. The key diagnostic test is an accurate intra-articular injection of the AC joint under ultrasound guidance. Surgical options include open excision or arthroscopic excision through superior or bursal portals. The procedure involves completely excising the inferior clavicle and osteophytes while preserving the postero-superior capsule to avoid instability. Thorough assessment and complete excision are important to address symptoms and avoid pitfalls like incomplete resection or post-









Acj excision watanabe india
- 1. AC Joint Excision Mr Chris Roberts Consultant Orthopaedic Surgeon Ipswich Hospital NHS Trust 2nd Indian Watanabe meeting, Chennai
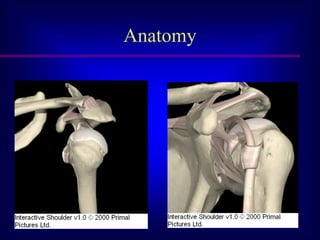
- 2. Anatomy • Diarthrodial joint • Two types of fibrocartilage discs : complete partial (meniscoid) • No function after 4th decade • Nerve supply : axillary suprascapular lateral pectoral
- 3. Anatomy
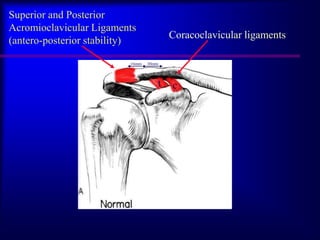
- 4. Superior and Posterior Acromioclavicular Ligaments Coracoclavicular ligaments (antero-posterior stability) 16mm 30mm t c
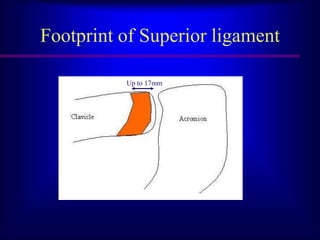
- 5. Footprint of Superior ligament Up to 17mm
- 6. ‘Normal’ x-rays Urist 100 shoulders : 49% clavicle over-riding acromion 27% vertical 21% incongruent 3% clavicle under-riding acromion
- 7. Correct operation done correctly Right reasons Full excision Safely
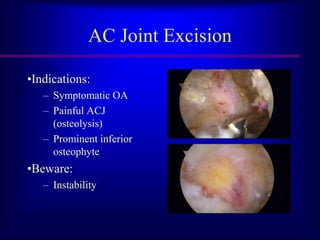
- 8. AC Joint Excision •Indications: – Symptomatic OA – Painful ACJ (osteolysis) – Prominent inferior osteophyte •Beware: – Instability
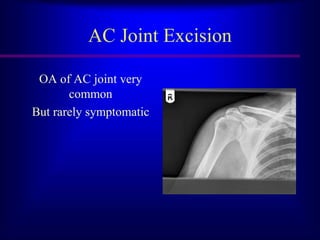
- 9. AC Joint Excision OA of AC joint very common But rarely symptomatic
- 10. AC Joint Excision OA of AC joint very common But rarely symptomatic SO Excision based on clinical findings
- 11. Examination
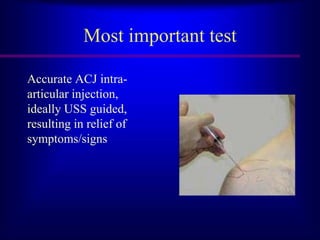
- 13. Most important test Accurate ACJ intra- articular injection, ideally USS guided, resulting in relief of symptoms/signs
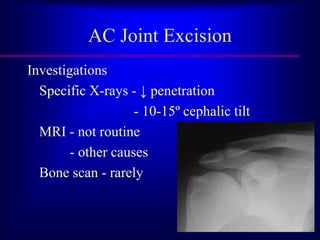
- 14. AC Joint Excision Investigations Specific X-rays - ↓ penetration - 10-15º cephalic tilt MRI - not routine - other causes Bone scan - rarely
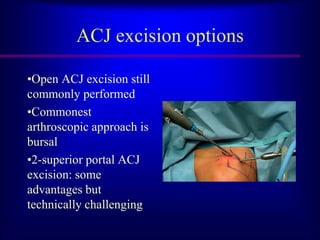
- 15. ACJ excision options •Open ACJ excision still commonly performed •Commonest arthroscopic approach is bursal •2-superior portal ACJ excision: some advantages but technically challenging
- 16. Set-up • Beach chair/lateral decubitus • Hypotensive anaesthesia • Radio-frequency device • 4.0 or 5.5mm acromionizer
- 19. Lateral and Neviaser viewing portal
- 20. Work to a pattern • Clear antero-inferior capsule and surrounding fat • Ensure correct resection depth by excising antero- inferior clavicle to depth of burr • Excise remaining inferior clavicle to same depth • Excise superior clavicle preserving superior capsule • Excise central bump
- 22. Inferior osteophyte without symptoms Co-plane osteophyte level with acromion or Excise whole depth of clavicle Avoid excision part clavicle depth
- 23. Pitfalls •Incomplete excision – Posterior – Superior osteophyte •Instability
- 24. Summary • Assess clinically – decision before operation • Vary portals for good view • Work to a pattern • Preserve postero-superior capsule
- 25. AC Joint Excision Thank you