
















Acute burn induced coagulopathy
- 1. BLSA Trainee Prize Day 07 Aug 2012 Tapiwa Kundishora ┬¦, Peter Sherren┬¦ Joseph Hussey*, Rabecca Martin*, Bruce Emerson* Mike Parker~ ┬¦ST6/7 Anaesthesia *Consultant Anaesthetist ~Statistician- Anglia Ruskin University
- 2. Introduction ’éŚ Coagulopathy in trauma is multifactorial; Hypothermia, acidosis, dilutional coagulopathy, pre- existing bleeding diathesis, Disseminated Intravascular Coagulation ’éŚ Acute Traumatic Coagulopathy (ATC) demonstrated by Brohi et al in 25 % of injured patients. ’éŚ ATC is associated with a higher mortality. ’éŚ Coagulopathy in burns patients also exists but is less well understood ’éŚ The presence of coagulopathy impacts in early burn excision and grafting.
- 3. Discussion Mechanisms of Coagulopathy in Trauma
- 4. Aim ’éŚ To determine the incidence of acute burn induced coagulopathy (ABIC) in burns patients ’éŚ To determine whether ABIC has any significance in terms of patient outcomes ’éŚ To determine if ABIC is an independent predictor of mortality in burns patients
- 5. Methods ’éŚ Retrospective review medical records -St Andrews Burns and Plastics Centre Intensive Care Unit. Inclusion Criteria ’éŚ All patients admitted Jan 2006 to Dec 2011 ’éŚ Burns > 30 % Total Body Surface Area (TBSA)
- 6. Methods Exclusion Criteria ’éŚ admission Ōēź 12 hours after the burn, ’éŚ suspected cyanide poisoning ’éŚ pre-existing bleeding diathesis or receipt of anticoagulants ’éŚ blood product administration ’éŚ major non-thermal injuries ’éŚ medical skin loss ’éŚ Missing records
- 7. Definitions ’éŚ Acute Burn Induced Coagulopathy (ABIC): PT Ōēź14.6 s and/or APTT Ōēź 45 s (local lab. reference & Davenport et al) < 12 hours after thermal injury in patients included in our study. ’éŚ Abbreviated Burn Severity Index( ABSI) age, sex, Total Burnt Surface Area (TBSA), full thickness Burn, inhalational injury
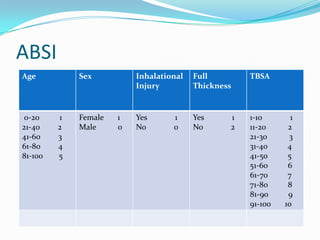
- 8. ABSI Age Sex Inhalational Full TBSA Injury Thickness 0-20 1 Female 1 Yes 1 Yes 1 1-10 1 21-40 2 Male 0 No 0 No 2 11-20 2 41-60 3 21-30 3 61-80 4 31-40 4 81-100 5 41-50 5 51-60 6 61-70 7 71-80 8 81-90 9 91-100 10
- 9. Methods ’éŚ Analysed for association between coagulopathy with demographics, Abbreviated Burn Severity Index ( ABSI) and fluid administration. ’éŚ Non parametric data- median (IQR). Mann Whitney U and FisherŌĆÖs exact tests ’éŚ Logistic regression modelling to assess prognostic value of a coagulopathy on the 28 day mortality rate. ’éŚ Analysis of data was performed using Microsoft Excel 2010 (Microsoft, USA) and program R (R Foundation for Statistical Computing, Austria) by a statistician. ’éŚ A p value < 0.05 was considered statistically significant.
- 10. Results total cases reviewed (n=205) excluded (n=60) missing data (n=28) Normal Clotting Acute Coagulopathy (n=71) (n=46)
- 11. Results
- 12. Results
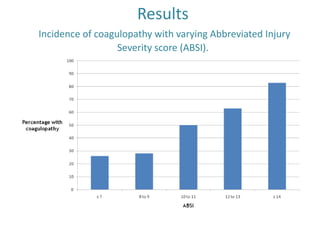
- 13. Results Incidence of coagulopathy with varying Abbreviated Injury Severity score (ABSI).
- 14. Results 28 day mortality in analysed patients
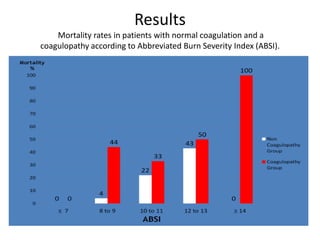
- 15. Results Mortality rates in patients with normal coagulation and a coagulopathy according to Abbreviated Burn Severity Index (ABSI).
- 16. Results Scatter plot of Prothrombin time versus Abbreviated Burn Severity Index (ABSI). Pearson product moment correlation coefficient r - 0.292 and p - 0.0013.
- 17. Results Scatterplot of Prothrombin time versus serum lactate Pearson product moment correlation coefficient r - 0.292 and p - 0.0013
- 18. Results Predictive value of ABIC ’éŚ Possible predictors of mortality assessed included coagulopathy and all the components of the ABSI (Age, sex, inhalational injury, full thickness burn and TBSA). ’éŚ The addition of an early coagulopathy to ABSI improved the goodness of fit for the 28 day mortality model from a R2 37.9% to 43.0% and a Scaled Brier score 26.6% to 29.5% (p ŌĆō 0.027). ’éŚ As an independent predictor of 28 day mortality, ABIC has an odds ratio (OR) of 3.42 (1.11-10.56).
- 19. Discussion ’éŚ Various derangements of coagulation in major burns patients has been described ’éŚ Most of the published work focuses on DIC and a delayed hypercoagulable state ’éŚ The incidence of DIC is variable. Barret et al 0.09 % incidence in 3331 patients Lavrentieva et al 41/45 patients ’éŚ Small number of patients overall in most( 5-60)
- 20. Discussion ’éŚ ABIC was present in 39.3% of our patients. Brohi et al showed an incidence of ATC of 25 % ’éŚ ABIC was associated with severity and thickness of burn (ABSI) & inhalational injury. ’éŚ Acute Traumatic Coagulopathy is caused by endothelial damage & hypoperfusion leading to increased thrombomodulin expression ’éŚ Similar mechanisms are likely to be involved in burns patients
- 21. Conclusion ’éŚ In patients with major thermal injuries, ABIC exists. ’éŚ This coagulopathy correlates to serum lactate and ABSI but is unrelated to fluid administration. ’éŚ Mortality is higher in patients with ABIC ’éŚ ABIC may be an independent predictor of mortality, however a more robust study would be required to prove this. ’éŚ More research is required to evaluate clotting in burns patients using methods other than PT/APTT like thromboelastometry.
- 22. References 1. Brohi K, Singh J, Heron M, Coats T. Acute Traumatic coagulopathy. J Trauma. 2003;54:1127-1130. 2. Davenport R, Manson J, DeŌĆÖArth H, Platton S, Coates A, Allard S, Hart D, Pearse RM, Pasi J, MacCullum P, Stanworth S, Brohi K. Functional definition and characterization of acute traumatic coagulopathy. Crit Care Med. 2011;39(12):2652-2658. 3. Maegele M, Lefering R, Yucei N, Tjardes T, Rixen D,Paffrath T, Simanski C, Neugebauer E, Bouillon B; AG Polytrauma of the German Trauma Society (DGU). Early coagulopathy in multiple injury: an analysis from the German Trauma Registry on 8724 patients. Injury. 2007 Mar;38(3):298-304. 4. Firth D, Davenport R, Brohi K. Acute traumatic coagulopathy. Curr Opin Anaesthesiol. 2012 Apr;25(2):229-34. 5. Schlag G, Redl H. Mediators in Trauma. Act Anesthesiol Belg. 1987;31:281-291. 6. Vindenes HA, Ulvestad E, Bjerknes R. Concentrations of cytokines in plasma of patients with large burns: their relation to time after injury, burn size, inflammatory variables, infection, and outcome. Eur J Surg. 1988 Sep;164(9):647-56. 7. Latenser BA. Critical care of the burn patient: the first 48 hours. Crit Care Med. 2009 Oct;37(10):2819-26. 8. Lavrentieva A, Kontakiotis T, Bitzani M, Papaioannou-Gaki G, Parlapani A, Thomareis O, Tsotsolis N, Giala MA. Early coagulation disorders after severe burn injury: impact on mortality. Intensive Care Medicine. 2008 Apr;34(4):700-6. 9. King DR, Namias N, Andrews DM. Coagulation abnormalities following thermal injury. Blood Coagul Fibrinolysis. 2010 Oct;21(7):666-9. 10. Kowal-Vern A, Gamelli RL, Walenga JM, Hoppensteadt D, Sharp-Pucci M, Schumacher HR. The effect of burn wound size on hemostasis: a correlation of the hemostatic changes to the clinical state. J Trauma. 1992 Jul;33(1):50- 56; discussion 56-57. 11. Garcia-Avello A, Lorente JA, Cesar-Perez J, Garcia-Frade LJ, Alvardo R, Arevalo JM, Navarro JL, Esteban A. Degree of hypercoagulability and hyperfibrinolysis is related to organ failure and prognosis after burn trauma. Thromb Res. 1998 Jan;89(2):59-64. 12. Hendon DN. Total Burn Care. Vol 3. Saunders; 2003. 13. Roberts G, Lloyd M, Parker M, Martin R, Philip B,Shelley O, Dziewulski P. The Baux score is dead. Long live the Baux score: 27 year retrospective cohort study of mortality at a regional burns service. J Trauma. 2012;72(1):251-256. 14. Tobiasen J, Hiebert JM, Edlich RF. The abbreviated burn severity index. Ann Emerg Med. 1982 May;11(5):260-2. 15. Barret JP, Gomez PA. Disseminated intravascular coagulation: a rare entity in burn injury. Burns. 2005 May;31(3):354-7. 16. Kowal-Vern A, Sharp-Pucci MM< Walenga JM, Dries GJ, Gamelli RL. Trauma and thermal injury: Comparison of hemostatic and cytokine changes in the acute phase of injury. J Trauma. 1998 Feb;44(2):325-9.
Editor's Notes
- #2: a