


Acute Respiratory Infection Guidelines(ARI)__PRESENTATION[1].pptx
- 1. Policies And Guidelines For Acute Respiratory Infections In Children By T.Nkhoma
- 2. Learning outcomes ŌĆó Define ARI ŌĆó Understand the global and local prevalence of ARI ŌĆó Know the principles for managing ARI ŌĆó Apply the preventive measurers for ARI ŌĆó Understand the role of nurses in ARI management and control
- 3. PRESENTATION OUTLINE ŌĆó Introduction ŌĆó Prevalence of ARI ŌĆó Causes of ARI ŌĆó Classification of ARI ŌĆó Strategies in the management of ARI ŌĆó Prevention of ARI ŌĆó Complications ŌĆó Conclusion
- 4. Introduction ŌĆó Acute respiratory infections (ARI) are infections that affect the upper and lower respiratory tract. ŌĆó They can be mild , moderate and severe ŌĆó Most ARI are mild, self limiting viral infections ŌĆó Mortality rates due to ARI are high in Malawi hence the need to have guidelines that will help reduce incidences of morbidity and mortality ŌĆó The policies and guidelines for ARI in Malawi are based on WHO guidelines
- 5. Introduction- ct/d ŌĆó The guidelines provide an overview on handling of these infections ŌĆó The Malawi ARI guidelines includes COVID-19 management ŌĆó The ARI guidelines are also incorporated in the Integrated Management of Childhood Illnesses (IMCI) guidelines ŌĆó The guidelines focus on 5 key areas on management of ARI problems
- 6. PREVALENCE AND INCIDENCE OF ARI ŌĆó ARI is emerging as one of the leading causes of morbidity and mortality in developing countries ŌĆó ARI affects approximately 32.6% of children under the age of 5 years (MOH, 2020). ŌĆó Of the 12 million death occurring annually under 5 years of age, ARI constitutes 19% of these deaths ŌĆó 20 to 25% 0f ARI deaths occur in children less than 2months ŌĆó 50 to 60% occur in those under 1 year ŌĆó Nearly 25 % of outpatients visits and 15% of all hospital admissions are due ARI
- 7. PREVALENCE AND INCIDENCE OF ARI ŌĆó Pneumonia accounts for 5.4% of all illnesses ŌĆó A study done in Mangochi on prevealnce of ARI showed that the annual prevalence of ARI was at 32.6% and risk factors included malnutrition, increased household density and sibling with ARI (Cox. et.al 2017)
- 8. Causes of ARI ŌĆó Bacterial pathogens- accounts for 60% of all ARI. Common ones be ’ā╝Streptococcus pneumonia ’ā╝Haemophilus influenzae ŌĆó Viruses ŌĆó Candida
- 9. Classification of ARI ŌĆó Classified according to location and severity 1. Upper respiratory tract infections (URTIs) ŌĆó Common cold: Runny nose, congestion, cough, sore throat ŌĆó Pharyngitis: sore throat, fever, swollen tonsils ŌĆó Laryngitis: hoarseness, cough, sore throat ŌĆó Sinusitis: facial pain, nasal congestion, headache2.
- 10. Classification of ARI 2. Lower respiratory tract infections ( LRTIs) ŌĆó Pneumonia: cough, fever, chest pain, difficulty breathing ŌĆó Bronchiolitis: in children less than 2 years, - wheezing, cough, difficulty breathing, apnea in severe cases ŌĆó Asthma: wheezing, cough, chest tightness, shortness of breath
- 11. Strategies in management of ARI ŌĆó The Malawi ARI control program has been established to work towards management of ARI ŌĆó ItŌĆÖs main strategies include: ŌĆó 1. Integrated Management of childhood illnesses (IMCI)- ’ā╝This is the comprehensive approach to managing childhood illnesses including ARI ’ā╝Training healthcare workers on IMCI
- 12. Strategies in management of ARI ct/d 2. ARI Management guidelines -covers ’ā╝How to conduct assessment ’ā╝Classification of the ARI ’ā╝Treatment and referral criteria 3. Antibiotic therapy - ’ā╝Antibiotics are reserved for severe ARI ’ā╝The guidelines stipulates which antibiotic or antimicrobials to be used for a particular illness ’ā╝ e.g use of cotrimoxazole as first line drug in pneumonia treatment
- 13. Strategies in management of ARI ct/d 4. Oxygen therapy- ’ā╝providing oxygen for children with severe ARI and hypoxemia ’ā╝ Ensuring availability of oxygen concentrators and cylinders in health facilities 5. Fluid Management- ’ā╝oral rehydration therapy for mild ,moderate ’ā╝intravenous fluids for severe dehydration and those unable to drink
- 14. Strategies in management of ARI ct/d 6. Vaccination ŌĆō ’ā╝ vaccines for preventable ARI e.g Pneumoccocal conjugate vaccine (PCV). 7. Community based care ’ā╝Community healthcare workers (CHWs) are trained to identify, manage ARI cases ’ā╝Provide support education and support to caregivers
- 15. Strategies in management of ARI ct/d 8. Referral Criteria
- 16. Case management of ARI ŌĆó Assess the child ŌĆó Classify the illness ŌĆó Decision for treatment ŌĆó Follow up cases
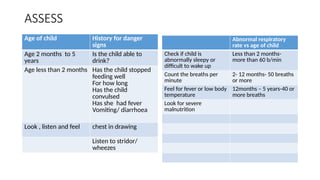
- 17. ASSESS Age of child History for danger signs Age 2 months to 5 years Is the child able to drink? Age less than 2 months Has the child stopped feeding well For how long Has the child convulsed Has she had fever Vomiting/ diarrhoea Look , listen and feel chest in drawing Listen to stridor/ wheezes Abnormal respiratory rate vs age of child Check if child is abnormally sleepy or difficult to wake up Less than 2 months- more than 60 b/min Count the breaths per minute 2- 12 months- 50 breaths or more Feel for fever or low body temperature 12months ŌĆō 5 years-40 or more breaths Look for severe malnutrition
- 18. CLASSIFY and Manage ŌĆó Based on the clinical manifestation conditions are classified as ŌĆó Mild ŌĆó Moderate ŌĆó Severe ŌĆó Management ŌĆó Home care for mild illness ŌĆó Hospitalization for moderate and severe cases ŌĆó Antimicrobial therapy ŌĆō oral or intravenous based on child condition ŌĆó Fluid management ŌĆó Oxygen therapy ŌĆó Manage fever ŌĆó Follow up care
- 19. Home care ŌĆó Mother or caregiver should ŌĆó Keep baby/child warm ŌĆó Continue b/feeding ŌĆó Increase feeding as recovery occurs ŌĆó Teach on dangers signs ŌĆó Adherence to prescribed drugs ŌĆó Review after 2 days or if no change in condition ŌĆó Home made therapies ŌĆó Use of humidified air
- 20. PREVENTION OF ARI ŌĆó Health education to parents and general population on ARI ŌĆó Breastfeeding infants exclusively for the first 6 months of life ’ā╝ boost their immune response to infections ’ā╝Reduce incidences of diarrhea diseases and malnutrition ŌĆó Feeding children with nutritious foods to keep the immune system strong ŌĆó Infection prevention practices ’ā╝Hand hygiene, social distance, cough etiquette, avoid overcrowding
- 21. PREVENTION OF ARI ŌĆó Avoid irritation of the respiratory tract by ’ā╝Indoor pollution from smoke (fire, cigarette, cowdung ŌĆó Immunization ’ā╝Haemophilis influenza B ’ā╝Pneumoccocal conjugate vaccine (PCV) ’ā╝DPT ’ā╝Measles ’ā╝BCG
- 22. Role of nurse midwife Discussion
- 23. CONCLUSION ŌĆó Acute respiratory infections are a major cause of illness and death among children under 5 years of age. ŌĆó The application of appropriate preventive measures, correct case management, health education at community level can help reduce morbidity and mortality ŌĆó Nurses should take a leading role in the identification, management and prevention of ARI
- 24. REFERENCE ŌĆó Cox. M. et al, ( 2017). The Prevelance and risk factors for Acute respiratory Infections in children aged 0-59 months in rural Malawi: A cross sectional study. Influenza other respir viruses. 2017 Nov;11(6): 489-496. ŌĆó WHO, (2020). Basic Principles for control of Acute respiratory infections in children in developing countries. A joint WHO/UNICEF Statement