






















ANALGESIA IN OBSTETRICS
- 1. LESSON PLAN ON ANALGESIA AND ANAESTHESIA IN OBSTETRICS PRESENTED BY, MS. MILAN SAWANT, 1ST YEAR M.Sc. NURSING, SAMARTH NURSING COLLEGE, DERVAN
- 2. DEFINITION OF PAIN ïPAIN IS A SUBJECTIVE EXPERIENCE, AND IT IS WHATEVER THE WOMAN SAYS IT IS FOR HER.
- 6. FATIGUE
- 7. CULTURAL AND SOCIAL FACTORS
- 8. EXPECTATIONS
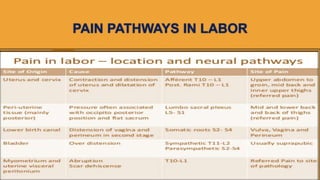
- 9. PAIN PATHWAYS IN LABOR
- 15. HYDROTHERAPY
- 19. REGIONAL ANALGESIA IN OBSTETRICS ïEPIDURAL ANALGESIA ï SPINAL ANALGESIA/ ANESTHESIA ïPATIENT CONTROLLED EPIDURAL ANALGESIA
- 21. CONTRAINDICATIONS FOR EPIDURAL ANAESTHESIA ï PATIENT REFUSAL OR INABILITY TO COOPERATE . ï INCREASED INTRACRANIAL PRESSURE SECONDARY TO A MASS LESION. ï SKIN OR SOFT TISSUE INFECTION AT THE SITE OF NEEDLE PLACEMENT ï FRANK COAGULOPATHY. ï UNCORRECTED MATERNAL HYPOVOLEMIA (E.G., HEMORRHAGE) . ï INADEQUATE TRAINING IN OR EXPERIENCE WITH THE TECHNIQUE .
- 23. CONTâĶ.. ïSPINAL ANESTHESIA INVOLVES THE INJECTION OF A LOCAL ANESTHETIC DIRECTLY INTO THE SPINAL FLUID, PROVIDING ANESTHESIA FOR VAGINAL OR LATE IN THE SECOND STAGE, WHEN THE FETAL HEAD IS ON THE PERINEUM. IT HAS NO EFFECT ON MATERNAL OR FETAL RESPIRATIONS BUT MAY CAUSE TEMPORARY HYPOTENSION AND A POSTSPINAL MATERNAL HEADACHE.
- 25. CONTâĶ.. ïPCEA HAS BEEN ASSOCIATED WITH GREATER MATERNAL SATISFACTION AS COMPARED WITH BOTH INTERMITTENT BOLUS INJECTION AND CONTINUOUS EPIDURAL INFUSION. ï PCEA RESULTS IN A LOWER AVERAGE HOURLY DOSE OF BUPIVACAINE THAN DOES A CONTINUOUS EPIDURAL INFUSION OF BUPIVACAINE. ïRESERVED FOR PATIENTS WHO ARE WILLING AND ABLE TO UNDERSTAND THAT THEY ARE IN CONTROL OF THEIR ANALGESIA.