




Anastomosis
- 2. ANASTOMOSIS DR ADEEL RIAZ PGR GEN SURGERY CPTH, LAHORE.
- 3. ANASTOMOSIS ? The word anastomosis comes from the Greek ĄŪanaĄŊ, without, and ĄŪstomaĄŊ, a mouth, re?ecting the joining of a tubular viscous (bowel) or vessel (usually arteries) after a resection or bypass procedure.
- 4. ANASTOMOSIS OF BOWEL Essentials for safe bowel anastomosis Local ? Good blood supply (no tension) ? Inverting anastomosis with appropriate suture ? Accurate apposition and suture technique (or stapling) ? Avoidance of tissue damage by clamps
- 5. ANASTOMOSIS OF BOWEL Essentials for safe bowel anastomosis Systemic ? Bowel preparation (and avoidance of spillage) ? Antibiotic prophylaxis ? Maintenance of good perfusion and tissue oxygenation during anaesthesia (correction of shock) ? Adequate nutritional attention ? Adequate resectional margins (cancer or in?ammatory bowel disease) and avoidance of chemotherapy/radiotherapy
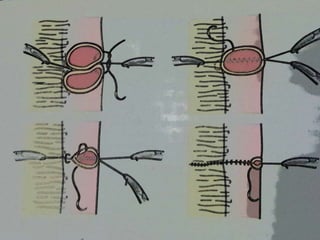
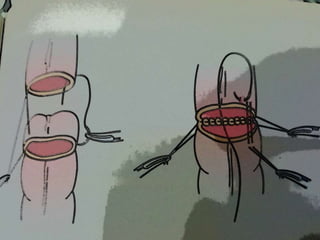
- 6. END TO END 2 LAYER TECHNIQUE PRINCIPLES ? The bowel ends must be brought together without tension. ? Stay sutures, which avoid the need for tissue forceps, may help with the placement of the posterior, continuous, seromuscular layer and allow rotation of the anastomosis. ? The inner continuous all-layers connell suture can be undertaken ?rst. An inverting seromuscular Lembert layer is then applied second. ? The apposition of bowel edges should, in each layer, be as accurate as possible. ? Bites should be approximately 5mm deep and 5mm apart.
- 8. END TO END 2 LAYER TECHNIQUE ? Suture materials should be of 2/0ĻC3/0 size and made of an absorbable polymer, mounted on an atraumatic round-bodied needle. ? ĄŪParachutingĄŊ or ĄŪpurse-stringingĄŊ a proximal dilated bowel lumen into narrower distal bowel risks a poor anastomosis and subsequent leakage. ? In such a case, a side-to-side or end-to-side anastomosis may be safer. ? The Cheatle split (making a cut into the anti- mesenteric border) may help to enlarge the lumen of distal, collapsed bowel.
- 10. END TO END 1 LAYER TECHNIQUE; END TO SIDE ANASTOMOSIS ? This interrupted single-layer extramucosal (seromuscular) suture is probably the most widely practised technique. ? They are useful in the following circumstances: ? when access is not easy, as in transabdominal oesophagogastric anastomoses or after low anterior resection; ? when there is disparity in the bowel lumen; ? when the bowel serosa is lacking.
- 12. INTESTINAL ANASTOMOSIS ? Ensure viable bowel ends before and after anastomosis ? Use atraumatic clamps if soiling is a risk ? Avoid risk to mesenteric vessels by clamps or sutures ? Synthetic polymers are the most conventional sutures for hand-sewn inverting anastomoses ? Interrupted and continuous suture techniques are comparably safe ? Disposable staple units are an alternative with safe inverting or everting anastomoses
- 13. ANASTOMOSIS OF VESSELS ? Vascular anastomosis require more precision than bowel anastomosis as they must be immediately watertight at the end of the operation when the clamps are removed. ? The intimal suture line must be as smooth as possible to minimize the risk of thrombosis and embolus, and regular to avoid leak. ? Suture size depends on vessel calibre: 2/0 is suitable for the aorta, 4/0 for the femoral artery and 6/0 for the popliteal to distal arteries. ? Microvascular anastomoses are made using a loupe and an interrupted suture down to 10/0 size.
- 14. ANASTOMOSIS OF VESSELS ? Polypropylene-like sutures with inde?nite integrity give the best results ? Intimal suture line must be smooth ? Knots must be secure ? Needle must pass from within outwards
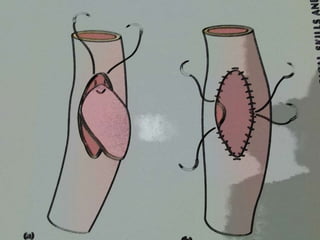
- 15. CLOSURE OF AN ARTERIOTOMY ? The vessel walls must be treated with care, particularly the intima, two single-ended sutures allow a knot to be placed externally at each end of the arteriotomy and a ?nal knot to be easily placed in the middle at the end of each side of the arterial closure. ? Vessels should always be sewn with the needle moving from in to out the lumen to avoid creating an intimal ?ap and to ?x any atherosclerotic plaque. ? The ?nal closure is made easily at the middle of the arteriotomy where the superior and inferior suture lines meet with the knot tied externally.
- 16. CLOSURE OF AN ARTERIOTOMY USING A VENOUS PATCH ? Once again, the suture line can be started at the top and bottom with a double-ended suture. ? The ?rst knot is then placed halfway along the edge of the suture line. ? The closure is completed with a ?nal knot on each side at the midpoint of the vein patch graft, using the inĻC out technique with ?xation of plaque and avoidance of damage to the intima using atraumatic forceps.
- 18. COMPLICATIONS ? Leakage ? Bowel ĻC peritonitis ? Vessel ĻC haematoma, haemorrhagic shock (early), pseudoaneurysm (late) ? Stenosis ? Bowel ĻC obstruction after ?brous stricture or disease recurrence ? Vessel (early and late) ĻC thrombosis, occlusion, gangrene
- 19. FACTORS AFFECTING ANASTOMOSIS HEALING Local ? Persisting disease process: cancer, chronic in?ammation ? Distal obstruction ? Poor blood supply: rectum, oesophagus ? Poor technical aspects: haematoma, dead space, poor perfusion ? Presence of foreign body ? Gross contamination/infection
- 20. FACTORS AFFECTING ANASTOMOSIS HEALING Systemic ? Shock of any cause ? Metabolic diseases: diabetes, uraemia, jaundice ? Immunosuppression: cancer, acquired immunode?ciency syndrome (AIDS), steroids ? Malnutrition: cancer
- 21. CONCLUSION ? Two of the most basic skills in surgery are suturing and knot tying. ? These techniques ought to be mastered before the surgeon in training enters the operating theatre. ? The surgical skills laboratory is the place to practise and master the techniques. ? Without practice, that skill will not developĄ..