
































ANATOMY OF NOSE AND PARANASAL SINUSES.pptx
- 1. ANATOMY OF PARANASAL SINUSES By Dr Kanav Rishi(PGT-1)
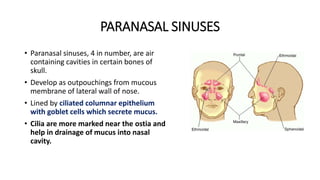
- 2. PARANASAL SINUSES • Paranasal sinuses, 4 in number, are air containing cavities in certain bones of skull. • Develop as outpouchings from mucous membrane of lateral wall of nose. • Lined by ciliated columnar epithelium with goblet cells which secrete mucus. • Cilia are more marked near the ostia and help in drainage of mucus into nasal cavity.
- 3. • Divided into 2 groups: • Anterior:- - Maxillary sinus - Frontal sinus - Anterior ethmoidal sinus • Posterior: - Posterior ethmoidal sinus - Sphenoid sinus
- 4. Development SINUS STATUS AT BIRTH FIRST RADIOLOGICAL EVIDENCE MAXILLARY PRESENT AT BIRTH 4- 5 MONTHS AFTER BIRTH ETHMOID PRESENT AT BIRTH 1 YEAR FRONTAL NOT PRESENT AT BIRTH 6 YEARS SPHENOID NOT PRESENT AT BIRTH 4 YEARS
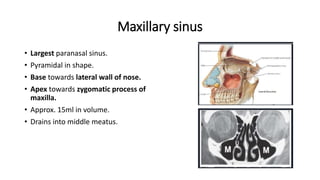
- 5. Maxillary sinus • Largest paranasal sinus. • Pyramidal in shape. • Base towards lateral wall of nose. • Apex towards zygomatic process of maxilla. • Approx. 15ml in volume. • Drains into middle meatus.
- 6. Relations • Anteriorly wall - Facial surface of maxilla, soft tissues of cheek • Posterior wall - Infratemporal and pterygopalatine fossa • Roof - Floor of orbit and is traversed by infraorbital nerves and vessels. • Floor - Alveolar and palatine processes of maxilla, 2nd premolar and 1st molar.
- 7. • Its Ostium is situated at the superior aspect of the medial wall. • The Nasolacrimal duct runs 4-9mm anterior to the ostium. • Fontanelles - Areas of bony dehiscence usually covered by mucosa present in the medial wall of maxillary sinus • Posterior fontanelle is patent in about 30% of cases and is called accessory ostium
- 8. Surgical anatomy • Consistent anatomical landmarks of PNS which helps during surgery include: • Maxillary sinus • Orbit from the maxillary sinus roof / orbital floor and medial orbital wall(lamina papyracea). • Skull base identified posteriorly by the sphenoid sinus. • These defined anatomical limits establish the boundaries of the paranasal surgical box including:- • (a) Horizontal component • (b) Vertical component
- 9. • HORIZONTAL COMPONENTS • Boundaries:- • Medially - Middle turbinate • Anteriorly - Medial orbital wall • Inferiorly - Floor of nose and • Superiorly - Skull base • VERTICAL COMPONENTS • Boundaries:- • Medially - Middle turbinate • Laterally - Lamina papyracea • Anteriorly - Nasofrontal beak • Posteriorly - Skull base
- 10. • Arterial supply - Infraorbital A and Greater Palatine A br of Int maxillary A • Venous drainage - Through pterygoid plexus and facial vein • Lymphatic drainage - Submandibular lymph nodes • Nerve supply - Infraorbital, Greater palatine and Superior alveolar nerves
- 11. Clinical importance • Dental caries or infection during tooth extraction may lead to spread of infection into the maxillary sinus. • Infraorbital canal may be dehiscent with nerve lying submucosally. • Accessory ostia if neglected during sinus surgery cause recirculation of mucus into maxillary sinus. • Endoscopic Sphenopalatine Artery Ligation • Endoscopic Maxillary Artery Ligation
- 12. Frontal sinus • Situated between inner and outer tables of frontal bone, above and deep to supraorbital margin • Asymmetric and loculated by incomplete septa. • Two sinuses separated by thin bony septum which sometimes may be absent. • Begins as frontal recess in 4th month of IUL. Frontal sinus
- 13. •Relations • Anteriorly - Related to skin over forehead • Posteriorly - Related to meninges and frontal lobe of brain • Inferiorly - Orbit and its contents • Drainage of the sinus is through frontal ostium into the frontal recess • The infundibulum leads into the frontal recess. • In sagittal section, the frontal infundibulum, frontal ostium and the frontal recess form “hour-glass configuration”
- 14. • The anterior ethmoidal cells may migrate anterosuperiorly into the frontal recess to produce different types of frontal cells: • Type I - A single cell above the agger nasi cell • Type II - Two or more cells above the agger nasi cell • Type III - large cell extending well into the frontal sinus mimicking the frontal sinus itself (frontal bulla) • Type IV - An isolated “loner cell” separately within the frontal sinus
- 15. Frontal recess • BOUNDARIES:- • Anteriorly:- Agger nasi and the frontal process of the maxilla, the frontal beak. • Medially:- Middle turbinate, the lateral lamella of the cribriform plate • Lateral:- Lamina papyracea • Posterior:- Upward continuation of the anterior face of the bulla.
- 16. • The uncinate process inserts onto the medial orbital wall in 85% of cases. • Thus, the frontal recess drainage pathway is medial to the uncinate process in 85% of cases. • An uncinate process with an isolated attachment to either the skull base or middle turbinate occurs in only 15% of cases. • Frontal drainage pathway located lateral to the uncinate process
- 17. Clinical importance • Acute rhinosinusitis (ARS):- Sudden, follows an URTI. • Chronic rhinosinusitis:- obstruct the frontal sinus outflow tract and lead to frontal pressure or headache. • ABRS:- Pott’s puffy tumour - Subperiosteal abscess of frontal sinus leads to headache, swelling and discharging frontal fistula. • Frontal sinus surgery:- The Agger nasi cell is key to all approaches to the frontal recess. • Balloon sinuplasty:- The technique introduces a balloon over a guide wire, in the sinus to unblock it.
- 18. • Osteomas:- slow growing tumours occur most often in the ethmoid followed by the frontal sinuses.(Gardner’s syndrome- multiple osteomas, colorectal polyps, skeletal abnormalities and supernumerary teeth) • Inverted papilloma:- After osteoma, the most frequent benign tumor of the frontal sinus. • Frontal pneumosinus dilatans:- An abnormally large aerated sinus. • Mucocele- Most common sinus involved is Frontal sinus.
- 19. Ethmoidal sinus • Most variable(3-18 cells on each side) and develop from pneumatisation of ethmoid bone • They occupy the space between upper third of lateral nasal wall medial wall of orbit • concha bullosa • Pneumatisation may occasionally extend beyond ethmoid bone
- 20. • Clinically, ethmoidal cells are divided by the basal lamella attachment into:- • Anterior ethmoid group • Posterior ethmoid group • BOUNDARIES: • Roof - fovea ethmoidalis • Medially - cribriform plate • Laterally - Lamina papyracea
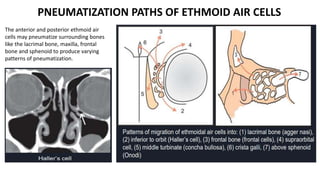
- 21. PNEUMATIZATION PATHS OF ETHMOID AIR CELLS
- 22. The anterior and posterior ethmoid air cells may pneumatize surrounding bones like the lacrimal bone, maxilla, frontal bone and sphenoid to produce varying patterns of pneumatization. PNEUMATIZATION PATHS OF ETHMOID AIR CELLS
- 23. • ANTERIOR GROUP • Agger nasi cell:- • Present in agger nasi ridge • Anterior most ant ethmoidal air cells • 1st prominent landmark encountered in FESS • Located ant-superior to insertion of middle turbinate • Haller cells(Infraorbital cells):- • Situated in the floor of orbit • Adhere to roof of maxillary sinus forms lateral wall of infundibulum. • Enlargement of this cell can impede the maxillary sinus drainage.
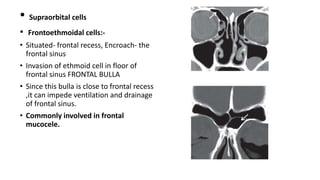
- 24. • Supraorbital cells • Frontoethmoidal cells:- • Situated- frontal recess, Encroach- the frontal sinus • Invasion of ethmoid cell in floor of frontal sinus FRONTAL BULLA • Since this bulla is close to frontal recess ,it can impede ventilation and drainage of frontal sinus. • Commonly involved in frontal mucocele.
- 25. • POSTERIOR GROUP • Lies posterior to the basal lamina. • 1-7 in number. • Open- superior meatus • Onodi cell:- • Posterior most cell • Supero-lateral to sphenoid sinus • Optic nerve and carotid artery is related to it laterally and there’s risk of injury during FESS.
- 26. • Bulla Ethmoidalis:- • Separated posteriorly from ground lamella by - retrobullar recess. • Separated from the base of the skull by -suprabullar recess • These together form a semilunar space above and behind the bulla- sinus lateralis of Grunwald • This sinus opens into the middle meatus by a semilunar cleft- hiatus semilunaris superioris.
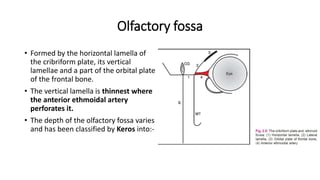
- 27. Olfactory fossa • Formed by the horizontal lamella of the cribriform plate, its vertical lamellae and a part of the orbital plate of the frontal bone. • The vertical lamella is thinnest where the anterior ethmoidal artery perforates it. • The depth of the olfactory fossa varies and has been classified by Keros into:-
- 28. Kero’s classification • TYPE 1 : 1-3mm • TYPE 2 : 4-7mm • TYPE 3 : 8-17mm • More the length of the lamella, more is the chance of the injury during surgery
- 29. • ARTERY SUPPLY • Anterior ethmoidal artery • Posterior ethmoidal artery • Sphenoid artery • VENOUS DRAINAGE • Anterior ethmoidal vein • Posterior ethmoidal vein
- 30. • NERVE SUPPLY • Anterior ethmoidal nerve • Posterior ethmoidal nerve • Orbital branch of pterygopalatine ganglion
- 31. Clinical importance • Acute rhinosinusitis:- Ethmoid sinus is the most common location. • Tumours:- Usually Adenocarcinomas. Most SCC of the sinonasal tract arises from the nasal cavity and ethmoid sinuses. • Aggressive psammomatoid ossifying fibroma (APOF) or juvenile-aggressive OF :- Most commonly affect the ethmoid sinus. • Fibrous dysplasia or Osteoma:- Causing secondary obstruction of drainage pathways, or mucocele of the sphenoid sinus.
- 32. • Allergic fungal sinusitis with the ethmoid sinuses with expansion of the sinus causing lamina papyracea remodelling. • Transcribriform Unilateral Access- The bone of the roof of the ethmoid sinus is removed to completely expose the dura.
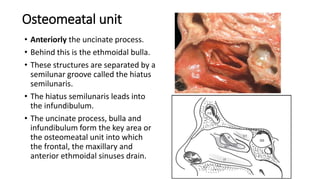
- 33. Osteomeatal unit • Anteriorly the uncinate process. • Behind this is the ethmoidal bulla. • These structures are separated by a semilunar groove called the hiatus semilunaris. • The hiatus semilunaris leads into the infundibulum. • The uncinate process, bulla and infundibulum form the key area or the osteomeatal unit into which the frontal, the maxillary and anterior ethmoidal sinuses drain.
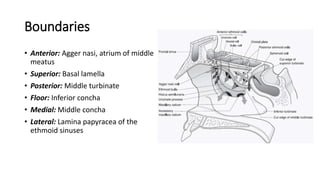
- 34. Boundaries • Anterior: Agger nasi, atrium of middle meatus • Superior: Basal lamella • Posterior: Middle turbinate • Floor: Inferior concha • Medial: Middle concha • Lateral: Lamina papyracea of the ethmoid sinuses
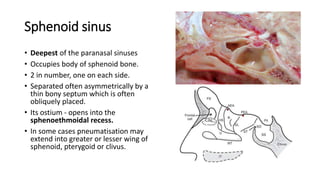
- 35. Sphenoid sinus • Deepest of the paranasal sinuses • Occupies body of sphenoid bone. • 2 in number, one on each side. • Separated often asymmetrically by a thin bony septum which is often obliquely placed. • Its ostium - opens into the sphenoethmoidal recess. • In some cases pneumatisation may extend into greater or lesser wing of sphenoid, pterygoid or clivus.
- 36. • RELATIONS: • ANTERIOR PART :- • Roof - Olfactory tract, optic chiasma and frontal lobe. • Laterally - Optic nerve, internal carotid artery, Maxillary nerve • POSTERIOR PART :- • Roof - Pituitary gland • Laterally - Cavernous sinus, ICA, CN 3,4,5,6 • Floor - Vidian nerve • This carotico-optic recess is extremely deep when ant clenoid process is pnuematised & optic nerve is dehiscent in such cases.
- 37. • ARTERIAL SUPPLY • Sphenopalatine A - Entire sinus except roof • Posterior ethmoidal A - Roof • VENOUS DRAINAGE • Via Maxillary veins into the jugular and pterygoid plexus system • NERVE SUPPLY • Nasociliary nerve - Roof • Branches of sphenopalatine nerve - Remaining sinus
- 38. Pneumatization • Position of sinus depend on extent of pnuematization • 3 types: • Conchal -Small pit in a predominantly non pneumatized sphenoid bone • Pre-sellar -Extending up to ant wall of sella turcica • Sellar -MOST COMMON • Mixed
- 39. Clinical importance • Pituitary fossa is present anterior and inferior to Sphenoid sinus and Intra- sphenoid sinus septum. • Visual pathway:- Optic nerves may be dehiscent of bone as they traverse the lateral wall of the sphenoid sinuses. • Removing all bony septations within the sphenoid sinus maximizes horizontal exposure, thus, providing access from lateral wall to lateral wall with clear visualization of the lateral optico-carotid recesses.
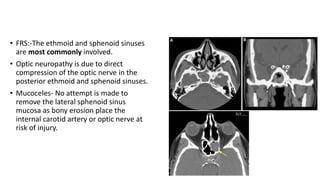
- 40. • FRS:-The ethmoid and sphenoid sinuses are most commonly involved. • Optic neuropathy is due to direct compression of the optic nerve in the posterior ethmoid and sphenoid sinuses. • Mucoceles- No attempt is made to remove the lateral sphenoid sinus mucosa as bony erosion place the internal carotid artery or optic nerve at risk of injury.
- 41. • Juvenile angiofibroma:- Sphenoid sinus floor are common hallmarks of JAs. Bony destruction of the sinus floor is followed by tumour extension into the sinus. • Epicenter of endonasal skull base approaches since it is often the starting point for endoscopic skull base experience.
- 42. THANK YOU