Annormalities of head size and shape
•Download as PPTX, PDF•
29 likes•10,138 views

This document discusses various abnormalities of head size and shape, including macrocephaly, microcephaly, and craniosynostosis. It defines each condition and lists potential causes. For macrocephaly, causes include megalencephaly, increased cerebrospinal fluid, enlarged vascular compartment, increased bony compartment, and miscellaneous lesions or diseases. Microcephaly can be primary/genetic or secondary/non-genetic, with various infectious, toxic, metabolic, or hypoxic-ischemic causes provided. Craniosynostosis involves premature fusion of cranial sutures, which can result in deformities like plagiocephaly or scaphocephaly. The document outlines approaches to diagnosis and
















Annormalities of head size and shape
- 1. Abnormalities of Head Size and Shape Mr.Riyaz Khan Aug-2012 Batch VI th Semster Department of Pediatrics Nepalgunj Medical College-Kohalpur
- 2. MACROCEPHALY • Definition: Head circumference ( occipito frontal ) > 2 standard deviation(SD) above the mean for age and sex.
- 3. 1 SD = 1.25 CM Macrocephaly > 2 SD i.e. 2.5 cm Microcephaly < 3 SD i.e 3.75 cm Take 50 centile as base line
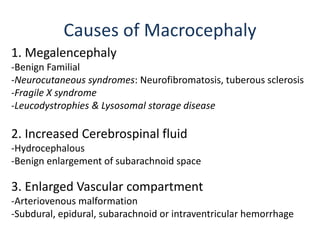
- 4. 1. Megalencephaly -Benign Familial -Neurocutaneous syndromes: Neurofibromatosis, tuberous sclerosis -Fragile X syndrome -Leucodystrophies & Lysosomal storage disease 2. Increased Cerebrospinal fluid -Hydrocephalous -Benign enlargement of subarachnoid space 3. Enlarged Vascular compartment -Arteriovenous malformation -Subdural, epidural, subarachnoid or intraventricular hemorrhage Causes of Macrocephaly
- 5. cont…. 4. Increase in bony compartment Bone disease: Achondroplasia, osteogenesis imperfecta, osteopetrosis Bone marrow expansion: Thalassemia major 5. Miscellaneous causes Intracranial mass lesions: Cyst, abscess or tumor Raised intracranial pressure: Idiopathic pseudotumor cerebri, lead poisoning, galactosemia
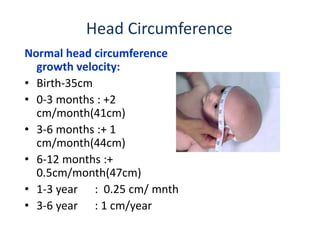
- 6. Head Circumference Normal head circumference growth velocity: • Birth-35cm • 0-3 months : +2 cm/month(41cm) • 3-6 months :+ 1 cm/month(44cm) • 6-12 months :+ 0.5cm/month(47cm) • 1-3 year : 0.25 cm/ mnth • 3-6 year : 1 cm/year
- 7. • History • Examination including auscultation of the skull for bruit • Developmental history • Rate of head growth – serial measurements Investigations : 1. Urea/electrolytes 2. Thyroid function test 3. Plasma amino acids 4. Urine amino acids and organic acids, glycosaminoglycans 5. CT head/MRI head preferably 6. Bone profile APPROACH
- 8. TREATMENT -generally require no tx - Infants with hydrocephalus may require neurological intervention( e.g. placement of a ventriculo-peritoneal shunt).
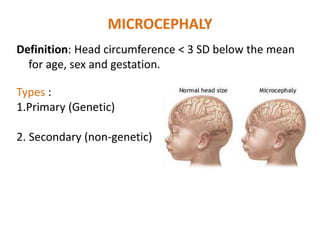
- 9. MICROCEPHALY Definition: Head circumference < 3 SD below the mean for age, sex and gestation. Types : 1.Primary (Genetic) 2. Secondary (non-genetic)
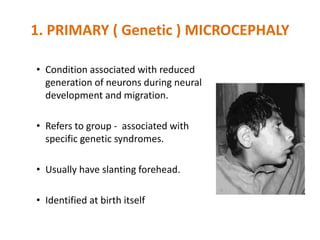
- 10. 1. PRIMARY ( Genetic ) MICROCEPHALY • Condition associated with reduced generation of neurons during neural development and migration. • Refers to group - associated with specific genetic syndromes. • Usually have slanting forehead. • Identified at birth itself
- 11. Causes for primary • Familial - AR • Autosomal dominant • Syndromes : 1. Down Syndrome 2. Cri du chat 3. Edward 4. Cornelia de Lange 5. Rubinstein Tyabi
- 12. • Results from noxious agents that may affect a fetus in utero or an infant during periods of rapid brain growth, particularly the first 2 years of life 2. Secondary ( non genetic) Microcephaly
- 13. 1. Radiation 2. Congenital infections – rubella, CMV, toxoplasmosis, HIV, Syphilis 3. Drugs – fetal alcohol, fetal hydantoin 4. Meningitis/encephalitis 5. Metabolic – maternal diabetes 6. Hypoxic ischemic encephalopathy 7. Malnutrition 8. Hyperthermia Causes for secondary microcepahaly
- 14. APPROACH • History (perinatal – family history) • Examination – dysmorphic features – malformations • Development • Growth – serial measurements of HC INVESTIGATIONS • Baseline biochemistry, metabolic screen • Genetic testing – karyotype, molecular genetics • TORCH screen • Ophthalmology • MRI brain
- 15. • No treatment for microcephaly • Baby’s head cannot be returned to a normal size & shape • According to the cause – Anticonvulsants – Physiotherapy – Hearing and speech therapy – Dietary management for failure to thrive – Genetic counseling Management
- 16. CRANIOSYNOSTOSIS Definition: premature fusion of one or more cranial sutures, either major(e.g metopic, coronal, sagittal, and lambdoid) or minor( frontnasal, temporosquamosal, and frontosphenoidal).
- 18. DEFORMITIES OF SKULL 1. Plagiocephaly 2. Scaphocephaly 3. Trigonocephaly 4. Turencephaly 5. Brachycephaly
- 19. -Fusion of either right or left side of the coronal suture -Causes the normal forehead and the brow to stop growing -Produces flattening of the forehead and the brow on the affected side, with the forehead tending to be excessively prominent on the opposite side PLAGIOCEPHALY
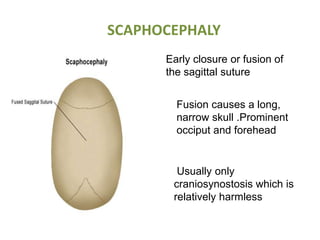
- 20. SCAPHOCEPHALY Early closure or fusion of the sagittal suture Fusion causes a long, narrow skull .Prominent occiput and forehead Usually only craniosynostosis which is relatively harmless
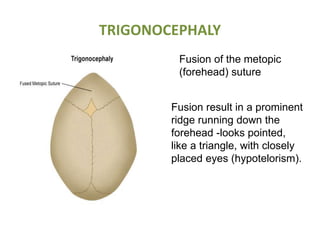
- 21. TRIGONOCEPHALY Fusion of the metopic (forehead) suture Fusion result in a prominent ridge running down the forehead -looks pointed, like a triangle, with closely placed eyes (hypotelorism).
- 22. • Turriencephaly – cone shaped head . Fusion of coronal and speno frontal or fronto ethmoid sutures. • Brachycephaly – premature closure of coronal suture expands skull parallel to coronal suture , thus broadening of forehead with short AP diameter. Eg – in many syndromes like Downs Syndrome
- 23. Diagnosis • Palpation of suture reveals prominent bony ridge. • Fusion may be confirmed by x-ray skull • Associated syndromes – Crouzon , Alperts, Carpenter
- 24. Management • Premature fusion of single suture rarely causes any neurological deficit . Thus, in this situation the only indication is cosmetics. • 2 or more suture fusion – more complications eg. ↑ ICT, hydrocephalus, optic atrophy, DNS, choanal atresia --- operative surgery essential – craniectomy with craniofacial correction. • Usually good prognosis with non syndromic infants……………
- 25. Thank You