Antiasthmetic drug
- 1. Mrs Khushbu K. Patel Asst. Professor
- 2. INTRODUCTION
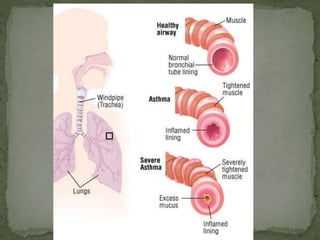
- 3. Chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. In susceptible individuals, this inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are associated with widespread but variable airflow obstruction that is reversible either spontaneously, or with treatment.
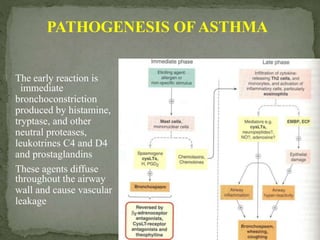
- 6. PATHOGENESIS OFASTHMA The early reaction is immediate bronchoconstriction produced by histamine, tryptase, and other neutral proteases, leukotrines C4 and D4 and prostaglandins These agents diffuse throughout the airway wall and cause vascular leakage
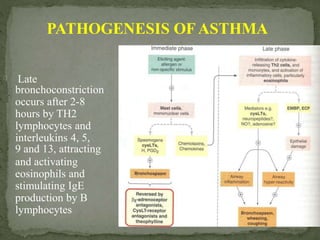
- 7. PATHOGENESIS OFASTHMA Late bronchoconstriction occurs after 2-8 hours by TH2 lymphocytes and interleukins 4, 5, 9 and 13, attracting and activating eosinophils and stimulating IgE production by B lymphocytes
- 8. Ąö Allergens Ąö Dust mites, mold spores, animal dander, cockroaches, pollen, indoor and outdoor pollutants, irritants (smoke, perfumes, cleaning agents). Ąö Pharmacologic agents; ASA, beta-blockers. Ąö Physical triggers (exercise, cold air, distilled water, and sulfur dioxide) Ąö Diseases; GERD, viral and bacterial URI, rhinitis Ąö Physiologic factors
- 9. Global Initiative for Asthma (6-point plan) Ąö Educate patients to develop a partnership in asthma management Ąö Assess and monitor asthma severity with symptom reports and measures of lung function as much as possible Ąö Avoid exposure to risk factors Ąö Establish medication plans for chronic management in children and adults Ąö Establish individual plans for managing exacerbations Ąö Provide regular follow-up care
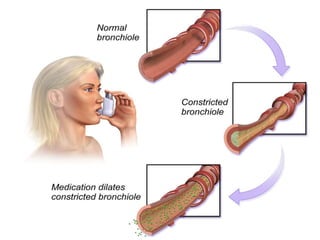
- 11. ? Asthma attacks are due to release of various mediators and other condition. ? Various classes of agents are available for treatment of asthma. ? Drugs used for asthma can be administrated by inhalation because, ? Enhance therapeutic effects ? Minimize systemic effects ? Rapid relief of acute attacks ? 2 type inhalation are used: (1). Dry Powder inhalers (2). Nebulizers
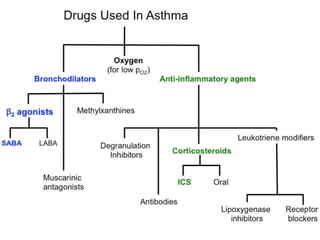
- 13. A) Short term relievers used for relief of acute bronchodilators: 1. Beta Adrenergic agonists 2. Methylxanthines/Phosphodiesterase inhibitors 3. Anrimuscrinic agents B) Long term controllers for reduction of symptoms and prevention of attacks: 1. Corticosteroids 2. Leukotriene pathway antagonists 3. Inhibitors of mast cell degranulation
- 14. 1. Beta Adrenergic agonists: (i) Drugs acting on both ĶÂ1 and ĶÂ2receptors: Epinephrine Ephedrine Isoproterenol ii) Beta2 selective drugs: Albuterol Terbutaline Metaproterenol Pirbuterol Bitolterol Salmoterol Formoterol
- 15. MECHANISM OF ĶĒ-ADRENERGIC RECEPTOR ? ĶÂ receptors are the predominant receptors in bronchial smooth muscle. Selective ĶÂ2 agonist are now widely used for treatment of asthma. Stimulate adenylyl cyclase, which leads to relaxation of bronchial smooth muscle and inhibition of release of mediators of immediate hypersensitivity. . which increases synthesis of cAMP Inhibits release of mast cell mediators such as histamine, leukotrienes, and prostaglandin-D2.
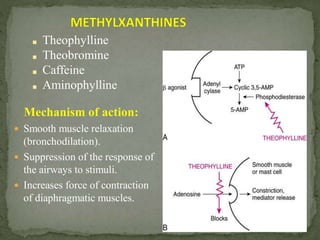
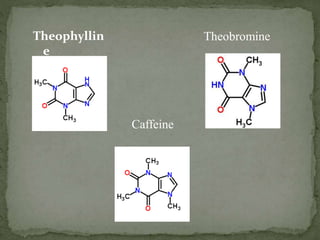
- 17. ? Smooth muscle relaxation (bronchodilation). ? Suppression of the response of the airways to stimuli. ? Increases force of contraction of diaphragmatic muscles. Ąö Theophylline Ąö Theobromine Ąö Caffeine Ąö Aminophylline Mechanism of action:
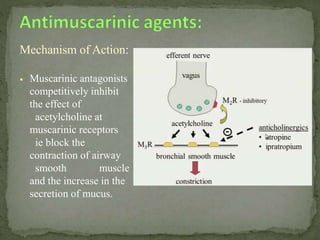
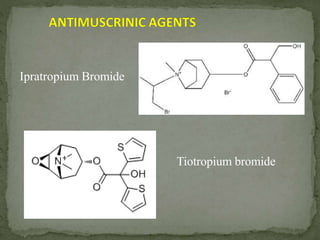
- 19. Mechanism of Action: ? Muscarinic antagonists competitively inhibit the effect of acetylcholine at muscarinic receptors ie block the contraction of airway smooth muscle and the increase in the secretion of mucus.
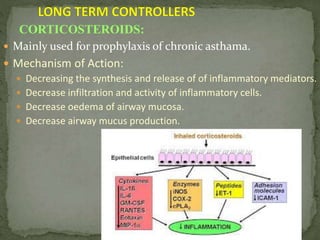
- 21. ? Mainly used for prophylaxis of chronic asthama. ? Mechanism of Action: ? Decreasing the synthesis and release of of inflammatory mediators. ? Decrease infiltration and activity of inflammatory cells. ? Decrease oedema of airway mucosa. ? Decrease airway mucus production. CORTICOSTEROIDS:
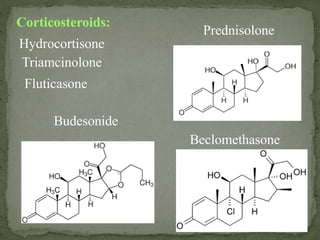
- 22. Corticosteroids: Prednisolone Hydrocortisone Beclomethasone Triamcinolone Fluticasone Budesonide
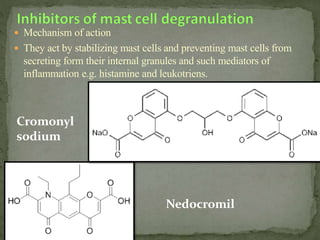
- 25. ? Mechanism of action ? They act by stabilizing mast cells and preventing mast cells from secreting form their internal granules and such mediators of inflammation e.g. histamine and leukotriens. Nedocromil Cromonyl sodium