









Approach of patient with breathing difficulties
- 1. APPROACH OF PATIENT WITH BREATHING DIFFICULTIES Dr PJCA Mbizi Family medicine October 2018
- 2. introduction Ō¢Ā Acute breathlessness is a common emergency condition .the effort required for breathing often makes it virtually impossible for the patient to provide any form of medical history and questioning may only make the situation worse.The clinician s skills will help to determine the underlying cause and dictate appropriate management .
- 3. Immediately life threatening causes and signs of breathlessness Ō¢Ā airway assessment Ō¢Ā Breathing assessment Ō¢Ā Circulation assessment Ō¢Ā NB it is important to remember that the breathless patient does not always have pathological arising primarily from the respiratory or cardiovascular systems
- 4. 1 . AIRWAYASSESSMENT Ō¢Ā Airway problem are common in acute emergencies Ō¢Ā Airway obstruction is the immediately life threatening problem due to : Ō¢Ā Pharynx ; tongue swelling, swelling of the epiglottis or soft tissue Ō¢Ā Larynx : oedema, spasm of the vocal cords, foreign body, trauma Ō¢Ā Subglottic: secretions or foreign body , swelling Ō¢Ā Bronchial : aspiration, tension pneumothorax, foreign body
- 5. Primary assessment and resuscitation Ō¢Ā Look at the chest for the rate, depth and symmetry of movement ,look in the mouth for blood , gastric contents, frothy sputum (pulmonary edema) and foreign body Ō¢Ā Listen for breath sounds , partial obstruction maybe as inspiratory noises indicates upper airway obstruction ( stridor), expiratory noises for lower airway obstruction (wheezing ), crowing (laryngeal spasm) , gurgling or snoring Ō¢Ā Feel for expired air, chest movement ,position of the trachea, any subcutaneous emphysema Ō¢Ā Airway control and ventilation are essential prerequisites for successful management of the acutely ill, airway obstruction should be recognized and managed immediately, endotracheal intubation remains the best method of securing and controlling the airway, but requires additional equipment, skill and practice.
- 6. Summary of airway assessment Ō¢Ā Look respiratory rate , effort , symmetry Ō¢Ā Feel expired air, trachea Ō¢Ā Listen : count to 10 , breath sounds, added noises Ō¢Ā Resuscitation :high concentrations of inspired oxygen may relieve some of the patients s distress. If airway obstruction is suspected, request IMMEDIATE review by a specialist. If a foreign body has been inhaled, attempt a Heimlich or modified Heimlich manoeuvre
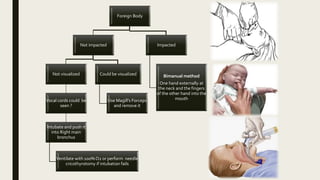
- 8. Foreign Body Not impacted Not visualized Vocal cords could be seen ? Intubate and push it into Right main bronchus Ventilate with 100% O2 or perform needle cricothyrotomy if intubation fails Could be visualized Use MagillŌĆÖs Forceps and remove it Impacted Bimanual method One hand externally at the neck and the fingers of the other hand into the mouth
- 9. Assess consciousness If Crying/Coughing : encourage coughing Unable to cough- HeimlichŌĆÖs maneuver If unconscious Basic airway support Direct laryngoscopy and Magill forceps If unsuccessful, insert an ETT and push into the right mainstem bronchus
- 10. 2. Breathing assessment Ō¢Ā Look for the color (pallor or well colored =mucus), posture, respiratory rate , effort , symmetry Ō¢Ā Feel for trachea position , chest expansion Ō¢Ā Percuss and listen : anterior and posterior aspects of both lungs in the upper, middle and lower zones. Ō¢Ā Resuscitation : if bronchospasm is suspected, treat patients with oxygen driven nebulized bronchodilators irrespective of the underlying cause, whilst clues to the cause are sought, immediate management of a tension pneumothorax is needle - followed by intravenous access and chest drain insertion.
- 11. 3. Circulation assessment Ō¢Ā Look for pallor, sweating, venous pressure Ō¢Ā Feel for pulse , rate ,rhythm and character, capillary refill time, blood pressure,apex beat Ō¢Ā Listen for blood pressure , heart sounds, extra sounds , lung bases Ō¢Ā Resuscitation : all patients should receive high concentrations oxygen, be trated in a seated position ( if level of consciousness permits) and have their oxygen saturation , pulse , blood pressure and cardiac rhythm monitored, intravenous acces is necessary and at least one large cannula (12-14 gauge) is required.The management of the shocked patient will depend on the underlying cause.Treatment options are as follow :
- 12. Shock management Ō¢Ā Acute, severe , left ventricular failure : inotropes, Ō¢Ā Dysrhytmia ( tachycardia= cardio-version, bradycardia = atropine, inotrope, pacing Ō¢Ā Hypo-voleamia : fluids Ō¢Ā Pulmonary embolus : anticoagulation, thrombolysis, fluids Ō¢Ā Sepsis :fluids, antibiotics, inotropes Ō¢Ā Anaphylaxis : adrenaline, fluids , chlorpheniramine, hydrocortisone Ō¢Ā Cardiac tamponade : fluids, pericardio-centesis
- 13. Secondary assessment Ō¢Ā Once the patient s conditions is stabilized and the primary assessment completed, further information can be obtained from the secondary assessment Ō¢Ā Summary : in the breathless patient , the immediately life threatening problem are ; Ō¢Ā Airway : obstruction Ō¢Ā Breathing : acute severe asthma, acute exacerbation of COPD, pulmonary edema, tension pneumothorax, critical oxygen desaturation Ō¢Ā Circulation : acute severe left ventricular failure, dysrhythmia, hypovolemia, pulmonary embolus, cardiac tamponade These conditions can be identified and differentiated clinically. all patients require oxygen and IVI access .
- 14. Secondary assessment Ō¢Ā Any patients with breathless will be able to give a history, Ō¢Ā Potentially life threatening causes of breathless are : Ō¢Ā RESPIRATORY : Ō¢Ā asthma, Ō¢Ā acute or chronic respiratory failure, Ō¢Ā pulmonary edema, Ō¢Ā Simple pneumopathy Ō¢Ā Pneumonia Ō¢Ā Pleural infusion Ō¢Ā Pulmonary embolus Ō¢Ā NON RESPIRATORY : Ō¢Ā metabolic acidosis e.g diabetic ketoacidosis, salicylate overdose Ō¢Ā Hemorrhage Ō¢Ā Acute or chronic gastro-enteritis
- 15. case Ō¢Ā A old man with known ischaemic heart disease was admitted to the coronary care unit after becoming acutely breathless, he denied any chest pain or cough, the following physical signs were elicited: Ō¢Ā RR 26/min Ō¢Ā Fine inspiratory crackles wre heard at both bases Ō¢Ā Pulse rate 140/min and regular Ō¢Ā BP 80/50 mmhg Ō¢Ā what would be your immediate management ?
- 16. References Ō¢Ā Acute medical emergencies , the practical approach , sd edition Ō¢Ā SaracinoA (October 2007). "Review of dyspnoea quantification in the emergency department: is a rating scale for breathlessness suitable for use as an admission prediction tool?". Emerg Med Australas 19 (5): 394ŌĆō404. Ō¢Ā Mahler DA, ed. Dyspnea. Mount Kisco, N.Y.: Futura Publishing, 1990. Ō¢Ā Barker LR, Burton JR, Zieve PD, eds. Principles of ambulatory medicine. 2d ed. Baltimore:Williams &Wilkins, 1986.