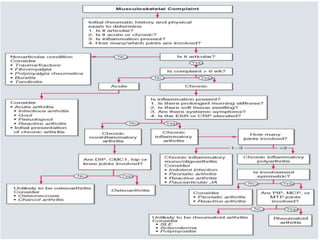





Approach to joint pains
- 1. CLINICAL APPROACH TO JOINT PAINS BY DR MAHESH GANDHI HOSPITAL GENERAL MEDICINE
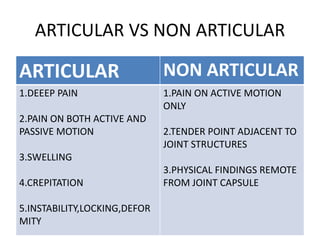
- 3. ARTICULAR VS NON ARTICULAR ARTICULAR NON ARTICULAR 1.DEEEP PAIN 2.PAIN ON BOTH ACTIVE AND PASSIVE MOTION 3.SWELLING 4.CREPITATION 5.INSTABILITY,LOCKING,DEFOR MITY 1.PAIN ON ACTIVE MOTION ONLY 2.TENDER POINT ADJACENT TO JOINT STRUCTURES 3.PHYSICAL FINDINGS REMOTE FROM JOINT CAPSULE
- 4. INFLAMMATORY VS NON INFLAMMATORY INFLAMMATORY N0N INFLAMMATORY 1.SIGNS OF INFLAMMATION{ERYTHEMA,WARMT H,PAIN,SWELLING}PRESENT 2.PROLONGED STIFFNESS 3.STIFFNESS IMPROVES WITH ACTIVITY 4.RAISED ACUTE PHASE REACTANTS 1.SIGNS OF INFLAMMATION ABSENT 2.SHORT DURATION STIFFNESS 3.INTERMITTENT STIFFNESS(GEL PHENOMENON) 4.NO RISE
- 5. HISTORY 1.AGE:YOUNG -SLE,REACTIVE ARTHRITIS MIDDLE- FIBROMYALGIA,RA ELDER- OA,POLYMYALGIA RHUEMATICA 2.SEX: MEN-GOUT,Spondylo Arthritis FEMALE-RA,FIBROMYALGIA,SLE 3.FAMILY H/O: GOUT,ANKY.SPONDYLITIS 4.DURATION: ACUTE-GOUT,SEPTIC ARTHRITIS CHRONIC-RA,OA MIGRATORY-RF,GONOCOOCAL,VIRAL ADDITIVE-RA,PSORIATIC ARTHRITIS
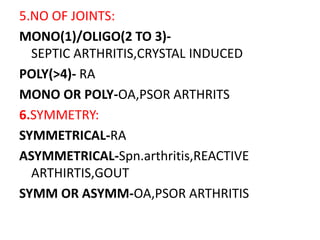
- 6. 5.NO OF JOINTS: MONO(1)/OLIGO(2 TO 3)- SEPTIC ARTHRITIS,CRYSTAL INDUCED POLY(>4)- RA MONO OR POLY-OA,PSOR ARTHRITS 6.SYMMETRY: SYMMETRICAL-RA ASYMMETRICAL-Spn.arthritis,REACTIVE ARTHIRTIS,GOUT SYMM OR ASYMM-OA,PSOR ARTHRITIS
- 7. 7.MANNER: UPPER EXTREMITY-RA,OA LOWER EXTREMITY-REACTIVE ARTHRITIS,GOUT AXIAL SKELETON-OA,ANK SPONDYLITIS,ONLY CERVICAL SPINE IN RA 8.PRECIPATATING FACTORS 9.COMORBIDITIES: GOUT-RENAL FAILURE MYELOMA-BACK PAIN
- 9. EXAMINATION EXAMINE TOTAL 28 JOINTS 1.Count number of tender joints 2.Count number of swollen joints 3.For swellings differentiate between joint effusions and bursal effusions by bulge sign 4.Assess joint stability by stabilising proximal joint and applying stress to distal appendage 5.Identify any subluxation/dislocations
- 10. 6.Inflammatory etiology will cause limited extension and joint will be in partial flexion (to decrease articular pressure).this results in flexion contractures. 7.Active and passive range motion of each joint should be done. hypermobility-marfans,EDS limited mobility - inflammtion,effusion,pain,deformity 8.Minor joint crepitus is common,but coarse crepitus is seen in OA 9.Look for joint deformity,muscle strenth