Approach to the diagnosis of dermatological disease
ŌĆóDownload as PPTX, PDFŌĆó
1 likeŌĆó363 views

How can I get a history of skin diseases from patients and perform physical examinations? Here you can easily learn.






























Approach to the diagnosis of dermatological disease
- 1. Approach to the DIAGNOSIS of DERMATOLOGICAL DISEASE Prepared and edited by: Associate prof. Dr. Khushhal Farooqi 2020 1
- 2. ŌĆśThe patient is the doctorŌĆÖs best tex Dermatologic diagnosis depends on the examinerŌĆÖs skill in skin inspection. 2
- 3. ŌĆó Exposure and lighting ŌĆó Patient must be properly gowned ŌĆó Extra lighting ŌĆó Always encourage the patient to undress completely; no peekaboo ŌĆó Develop a systematic approach and use it for every skin examination. ŌĆó Gently use your fingers to glide across the skin- your touch can ŌĆó One should do hand hygiene prior to and after touching the patient. How to perform a skin examination 3
- 4. 4
- 5. HISTORY OF CUTANEOUS DISORDERS ŌĆó A PROBLEM-FOCUSED HISTORY is sufficient for most common skin disorders. ŌĆó If, the patient has systemic complaints, or if diseases such as lupus erythematous or vasculitis are suspected, a DETAILED OR COMPREHENSIVE HISTORY may be needed. 5
- 6. 6
- 7. FITZPATRICK'S COLOR ATLAS AND SYNOPSIS OF CLINICAL DERMATOLOGY EIGHTH EDITION 2017 PHYSICAL EXAMIN Appearance ŌĆó Uncomfortable, ŌĆó toxic ŌĆó well. Vital Sign ŌĆó Pulse, ŌĆó Temperature ŌĆó Respiration Skin: learning to red 7
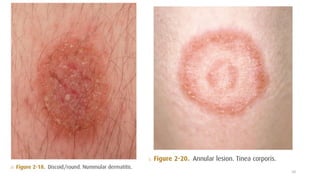
- 8. ŌĆ½┘Šž¦ž▒┘ćŌĆ¼ŌĆ½┘äŌĆ¼ ŌĆ½┘ŖžĄŌĆ¼ŌĆ½ž┤ž«ŌĆ¼ŌĆ½ž¬ŌĆ¼ ŌĆ½ž»ŌĆ¼ ŌĆ½┘Ŗ┘łŌĆ¼ŌĆ½ž║ŌĆ¼ŌĆ½ž¦┘åž▒┘łŌĆ¼ ŌĆ½ž»ŌĆ¼ ŌĆ½ž¬┌®█īŌĆ¼ŌĆ½ž│ŌĆ¼ŌĆ½┘Š┘łŌĆ¼ ŌĆ½ž»ŌĆ¼Prerequisites 1. Types of skin lesions 2. Colour 3. Margination 4. Consistency 5. Shape 6. ARRANGEMENT 7. DISTRIBUTION TYPES OF SKIN LESIONSŌĆ½┘Š┘Ŗ┌ś┘åž»┘äŌĆ¼ ŌĆ½ž¬┘łž▒┘łŌĆ¼ ŌĆ½ž¦┘ä┘üž©ž¦ŌĆ¼ ŌĆ½ž»ŌĆ¼ ŌĆ½┘ä┌®┘ćŌĆ¼ ŌĆ½ž»█īŌĆ¼ ŌĆ½ž»ž¦ž│█īŌĆ¼ 8
- 9. 9
- 10. 10
- 11. 11
- 12. 12
- 13. 13
- 14. 14
- 15. 15
- 16. 16
- 17. 17
- 18. Shaping Letters Into Words: Further Characterization of Identified Lesions 18
- 19. 19
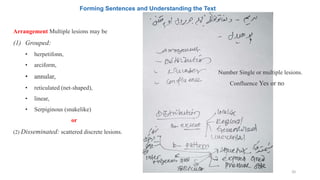
- 20. Forming Sentences and Understanding the Text Confluence Yes or no Number Single or multiple lesions. Arrangement Multiple lesions may be (1) Grouped: ŌĆó herpetifonn, ŌĆó arciform, ŌĆó annular, ŌĆó reticulated (net-shaped), ŌĆó linear, ŌĆó Serpiginous (snakelike) or (2) Disseminated: scattered discrete lesions. 20
- 21. 21
- 22. 22
- 23. Our Skin Is Covered With Invisible Stripes 23
- 24. 24
- 26. PRELIMINARY HISTORY This initial history is composed of two parts that correlate with the ŌĆó Chief complaint and ŌĆó The history of the present illness in the standard history format. 26
- 27. ’éĢ’ĆĀCHIEF COMPLAINT ŌĆó In eliciting the chief complaint, one can often learn much by asking an open-ended question, such as, ŌĆ£What is your skin problem?ŌĆØ ŌĆó This is followed by four general questions regarding the history of the present illness. 27
- 28. HISTORY OF THE PRESENT ILLNESS ŌĆó Onset and Evolution o ŌĆ£When did it start? o Has it gotten better or worse?ŌĆØ For most skin conditions, this is important information. ŌĆó Symptoms o ŌĆ£Does it bother you?ŌĆØ o ŌĆ£Does it itch?ŌĆØ. ŌĆó Treatment to Date ŌĆ£IŌĆÖve already tried that and it didnŌĆÖt work!ŌĆØ 28
- 29. REVIEW OF SYMPTOMS This should be done as Indicated by the clinical situation, with particular attention to possible connections between signs and disease of other organ systems (e.g., rheumatic complaints, myalgias, arthralgias, Raynaud phenomenon). 29
- 30. Review of Systems (ROS) A s k a b o u t ŌĆó Fever, chills, ŌĆó Fatigue, ŌĆó Weight changes, ŌĆó Lymphadenopathy, ŌĆó Joint pains, ŌĆó Wheezing, rhinitis, ŌĆó Menstrual history, ŌĆó Birth control methods, ŌĆó Depression, and anxiety. ŌĆó Additional ROS questions can be asked based on the patientŌĆÖs chief complaint. 30
- 31. EXAMINATION TOOLS 1. Potassium hydroxide mount 2. Culture 3. Biopsy ŌĆó The gold standard for precise diagnosis of many skin conditions remains tissue biopsy. The two most commonly employed techniques are shave biopsy and punch biopsy. 4. Magnification with hand lens. 5. Wood lamp (ultraviolet long-wave light) is valuable in the diagnosis of certain skin and hair diseases and of porphyria. With the Wood lamp (365 nm), 6. Diascopy 7. Dermoscopy , Digital dermoscopy 31
- 32. 32
- 33. 33
- 34. 34
- 35. 35