Back/Spine examination
44 likes12,217 views

Clinical examination notes of back/spine especially based on TU course of MBBS in Nepal.I hope many students will be helped with this notes.


































More Related Content
What's hot (20)
Similar to Back/Spine examination (20)




![musculoskeletal_system_examination[1] (1) (3).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/musculoskeletalsystemexamination113-241005064436-de0b77f1-thumbnail.jpg?width=560&fit=bounds)













Recently uploaded (20)




















Back/Spine examination
- 1. Back/Spine Examination Prepared by: Sunil Baniya Student, NAIHS-COM, sanobharyang, ktm, Nepal 1Knee Examination/ Sunil Baniya
- 2. • Adequate exposure is essential; patients must strip to their underclothes • Examination in standing, sittting and supine examination 1. LOOK – Gait Front – Posture – Forward bending – Lateral list
- 3. – Asymmetry of chest, pelvis – Scars, sinus – Leg shortening – Side – Kyphosis – Lordosis – Scars, sinus
- 4. Back - Tufts of hair - Café au laits spots - Paraspinal muscle spasm - Scars - Muscle wasting - scoliosis
- 5. 2. FEEL a. Temperature b. Tenderness: – Elicit spine tenderness by 3 methods i) Pressure over the interspinous area ii) Twisting or pressure over the paraspinous part (facet joint) = Spinous Rock iii) Thumping over vertebral column
- 6. 3. MOVE o Forward flexion: - Touching toes - Majority touches the ground - Touching mid tibia, 7 cm above the floor o Extension: normally 30° o Lateral flexion: try to touch each side of leg (Average = 30°) o Rotation: maximum 40° (first fix pelvis then only ask for rotation)
- 7. 4. MEASUREMENT: o To measure the lumbar excursion o Take any two bony points over the lumbar region 10 cm apart while standing upright o Measure the distance between that points when patient is asked to bend forward fully o The distance must be increased by at least 5 cm (i.e; lumbar excursion = 5cm) o If less than 3 cm, substantial pathology like ankylosing spondylitis
- 8. SPECIAL TESTS: 1. SLRT (Straight Leg Raising Test)/Sciatic stretch test/ Dural tension test 2. Well Leg Raise Test or Cross SLRT test 3. Bragard test 4. Lassegue’s test 5. Bowstring’s test 6. Patric test ( Faber sign) = for sacroiliac pathology
- 9. SLRT/ Sciatic Stretch Test/ Dural Tension Test: Method: o 1st do as active by patient himself o Confirm by passive method o Finding: test is +ve, if pain occurs between 30° – 70° of elevation o Back pain = central disc prolapse o Pain that radiates back to below knee, not just the thigh or back pain = lateral protrusion
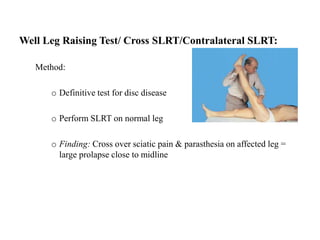
- 10. Well Leg Raising Test/ Cross SLRT/Contralateral SLRT: Method: o Definitive test for disc disease o Perform SLRT on normal leg o Finding: Cross over sciatic pain & parasthesia on affected leg = large prolapse close to midline
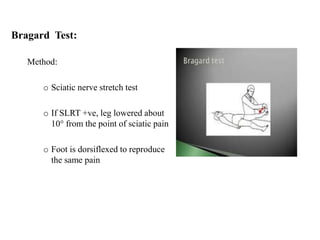
- 11. Bragard Test: Method: o Sciatic nerve stretch test o If SLRT +ve, leg lowered about 10° from the point of sciatic pain o Foot is dorsiflexed to reproduce the same pain
- 12. Lasegue’s Test: Method: o Patient supine o Thigh bent at 90° & knee bent at 90° o Gradually extend the knee keeping hip flexed o Thigh pain radiates down the leg = +ve
- 13. Bowstring’s Test: Method: o SLRT +ve o Slight flex the knee just to relieve pain o Then firmly press behind lateral hamstrings to tighten the common peroneal nerve o Radiating pain & parasthesia reappears o Finding: +ve Bowstring’s sign i.e; nerve root irritation
- 14. 5.NEUROLOGICAL EXAMINATION: L4 nerve: o Motor : grading of dorsiflexion o Sensory: medial aspect of the leg o Reflex: knee (normal/brisk/sluggish/absent) L5 nerve: o Motor: EHL (Extensor Hallucis Longus), plantiflexion, dorsiflexion of toe o Sensory : Anterolateral part of leg and dorsum of foot o Reflex: ankle jerk S1 nerve: o Motor: plantar flexion o Sensory: Lateral aspect of the sole o Reflex: ankle reflex
- 15. THANK YOU 15Knee Examination/ Sunil Baniya