Bcp inservice outreach linked in
ŌĆóDownload as PPTX, PDFŌĆó
1 likeŌĆó283 views

BrightStar offers private duty home care programs like HANDS and Clinical Pathways to reduce hospital readmissions and improve quality of life. HANDS provides home care after discharge to address issues that arise. Clinical Pathways is a condition-specific, transitional care program focused on reducing negative outcomes and optimizing quality of life through RN visits, education, and monitoring. These programs aim to address the top reasons for readmissions like medication management and lack of home support. They utilize technology, evidence-based practices, and specially trained staff to benefit patients, healthcare systems, and providers through better outcomes and efficiencies.






Bcp inservice outreach linked in
- 1. The Role of Private Duty Home Care in Reducing Hospital Readmissions & Enhancing Quality Of Life Taking Private Duty Home Care to a Whole New Level Hospital Assisted Nurse Discharge Service (HANDS) and BrightStar Clinical Pathways
- 2. The Opportunity ŌĆó Hospital/Health System As part of the Patient Protection & Affordable data will be scrutinized at a Care Act (PPACA), there number of levels and are a number of changes failure to achieve certain that will impact reimbursement to national CMS benchmarks hospitals and other will result in healthcare systems ŌĆō Financial Penalties ŌĆó Excessive Readmissions National efforts are underway to reduce ŌĆō Less Robust Rewards potentially preventable ŌĆó Poor Customer Satisfaction hospital readmissions and optimize the patient ŌĆó Poor Outcomes of Care experience
- 3. *Centers for Medicare & Medicaid Services, Public Affairs, April 2009 Medicare data shows that nearly 1 in 5 patients who leave the hospital are readmitted within the next month and that more than 75% of these Healthcare readmissions are preventable* systems need to look for new solutions since Research has demonstrated that many existing of the return trips can be prevented approaches are with an in-home care program not solving the that includes proper education and problem. supervision.
- 4. Top Reasons for 30-day hospital readmissions: ’ā╝ Failure to make follow-up appointments ’ā╝ Lack of communication ’ā╝ Failure to understand medication management ’ā╝ Absence of in-home support ’ā╝ Non-adherence to lifestyle recommendations ’ā╝ Failure to understand and actively participate in the management of their chronic disease
- 5. At BrightStar we utilize a Best Practice approach to care following the National Quality Standards of The Joint Commission
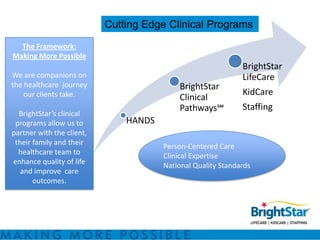
- 6. Cutting Edge Clinical Programs The Framework: Making More Possible BrightStar We are companions on LifeCare the healthcare journey BrightStar our clients take. KidCare Clinical PathwaysŌäĀ Staffing BrightStarŌĆÖs clinical programs allow us to HANDS partner with the client, their family and their Person-Centered Care healthcare team to Clinical Expertise enhance quality of life National Quality Standards and improve care outcomes.
- 7. BrightStarŌĆÖs Clinical Pathways ŌäĀ and HANDS Program was inspired by nationally recognized care transition programs: Coleman Care Transition Intervention Program which reduced hospital readmissions by 50% at 30, 60 and 90 days
- 8. HANDS is a transitional care program focused on a safe transition home ’é¦ After leaving the hospital it is important that the patient have a direct link to an accessible care provider. ’é¦ HANDS provides that link, bridging the transition to home and addressing issues and questions that arise. ’é¦ Medicare agencies may not be able to be there within the 1st - 24 hours and sometimes not for 2-4 days.
- 9. ŌĆó BrightStarŌĆÖs Hospital Accelerated Nurse Discharge Service (HANDS) is a transitional care program to facilitate a safe discharge home. ŌĆō It is ideally the beginning of a journey we take with the client and their healthcare team. HANDS: ŌĆó It begins at time of discharge and continues for a minimum of 24 hours ŌĆō critical transition time for What is it to re-engagement in the home setting. ŌĆó A visit by our Registered Nurse Care Our Manager is the cornerstone of the program ŌĆō Assessment, Medication Reconciliation, Disease Partners? State Education w/attention to Red Flag Symptoms ŌĆó Person-centered services performed by our CNA ŌĆō Transportation from hospital to home, Home Safety Check, Light Housekeeping, Retrieval of Simple Supplies (medications, groceries, etc), Light Meal Prep, Transition Check List which includes phone calls to loved ones, arranging/confirming follow-up appointment with discharging physician
- 11. ŌĆó HANDS Basic ŌĆō 3 hours CNA time HANDS Basic ŌĆō 1 RN Home Visit w/i 4-8 hours of Services hospital discharge ŌĆó HANDS Plus ŌĆō Everything included above ŌĆō Pre-discharge RN Visit at hospital (meet & greet, chart review, discharge instructions, etc) ŌĆō 1 additional RN visit ŌĆō 24/7 RN phone call availability for HANDS Plus 30 days Services ŌĆō Detailed medication instruction/med set-up if indicated
- 12. BrightStar Clinical Pathways Empowering individuals with chronic illness through our best practice approach
- 13. Simply putŌĆ” BrightStar Clinical Pathways ŌäĀ is a ŌĆōpatient centered ŌĆōcondition-specific ŌĆōtransitional care program Focused on ŌĆōreducing negative outcomes ŌĆōoptimizing quality of life
- 14. BrightStar Clinical Pathways SM ’é¦Patient Centered ’é¦Evidence-based ’é¦Condition-specific ’é¦Best practice approach ’é¦Time-limited (4 wks) ’é¦RN Clinical Pathway Coordinator ’é¦Specially Trained CNAs
- 15. BrightStar Clinical Pathways SM ’é¦ Heart failure ’é¦ COPD ’é¦ Pneumonia ’é¦ Acute MI ’é¦ Delirium & Dementia ’é¦ Diabetes ’é¦ Falls with Fracture
- 16. BrightStar Clinical PathwaysŌäĀ Materials
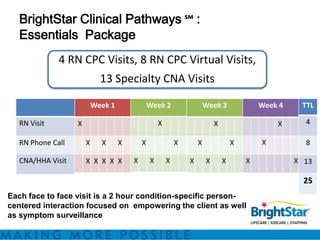
- 17. BrightStar Clinical Pathways ŌäĀ : Essentials Package 4 RN CPC Visits, 8 RN CPC Virtual Visits, 13 Specialty CNA Visits Week 1 Week 2 Week 3 Week 4 TTL RN Visit X X X X 4 RN Phone Call X X X X X X X X 8 CNA/HHA Visit X X X X X X X X X X X X X 13 25 Each face to face visit is a 2 hour condition-specific person- centered interaction focused on empowering the client as well as symptom surveillance
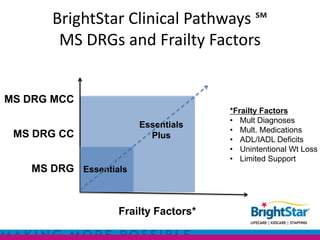
- 18. BrightStar Clinical Pathways ŌäĀ MS DRGs and Frailty Factors MS DRG MCC *Frailty Factors ŌĆó Mult Diagnoses Essentials ŌĆó Mult. Medications MS DRG CC Plus ŌĆó ADL/IADL Deficits ŌĆó Unintentional Wt Loss ŌĆó Limited Support MS DRG Essentials Frailty Factors*
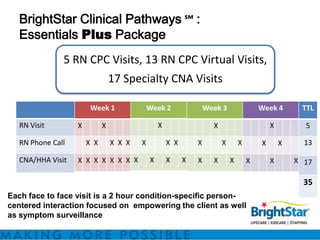
- 19. BrightStar Clinical Pathways ŌäĀ : Essentials Plus Package 5 RN CPC Visits, 13 RN CPC Virtual Visits, 17 Specialty CNA Visits Week 1 Week 2 Week 3 Week 4 TTL RN Visit X X X X X 5 RN Phone Call X X X X X X X X X X X X X 13 CNA/HHA Visit X X X X X X X X X X X X X X X X X 17 35 Each face to face visit is a 2 hour condition-specific person- centered interaction focused on empowering the client as well as symptom surveillance
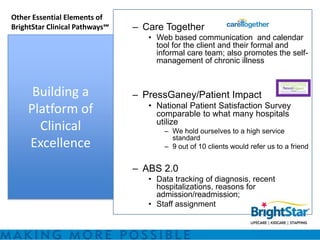
- 20. Other Essential Elements of BrightStar Clinical PathwaysŌäĀ ŌĆō Care Together ŌĆó Web based communication and calendar tool for the client and their formal and informal care team; also promotes the self- management of chronic illness Building a ŌĆō PressGaney/Patient Impact ŌĆó National Patient Satisfaction Survey Platform of comparable to what many hospitals utilize Clinical ŌĆō We hold ourselves to a high service standard Excellence ŌĆō 9 out of 10 clients would refer us to a friend ŌĆō ABS 2.0 ŌĆó Data tracking of diagnosis, recent hospitalizations, reasons for admission/readmission; ŌĆó Staff assignment
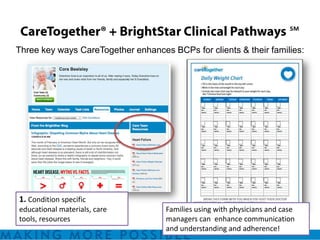
- 21. ŌäĀ Three key ways CareTogether enhances BCPs for clients & their families: 1. Condition specific educational materials, care Families using with physicians and case tools, resources managers can enhance communication and understanding and adherence!
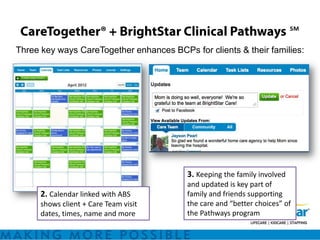
- 22. ŌäĀ Three key ways CareTogether enhances BCPs for clients & their families: 3. Keeping the family involved and updated is key part of 2. Calendar linked with ABS family and friends supporting shows client + Care Team visit the care and ŌĆ£better choicesŌĆØ of dates, times, name and more the Pathways program
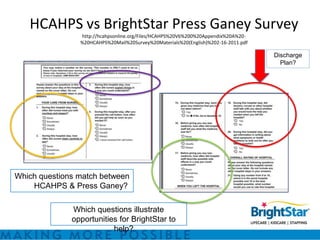
- 23. HCAHPS vs BrightStar Press Ganey Survey http://hcahpsonline.org/Files/HCAHPS%20V6%200%20Appendix%20A%20- %20HCAHPS%20Mail%20Survey%20Materials%20(English)%202-16-2011.pdf Discharge Plan? Which questions match between HCAHPS & Press Ganey? Which questions illustrate opportunities for BrightStar to help?
- 24. BrightStar Clinical Pathways ŌäĀ Foundational Concepts ŌĆó Person Centered ŌĆō The individual is more than the sum of their parts (or their diseases and medications) ŌĆó Patient Empowerment with Self Management of Chronic Disease ŌĆó BrightStar Clinical PathwayŌäĀ Team Leader ŌĆō Together ŌĆō Everyone ŌĆō Achieves ŌĆō More
- 25. Key BrightStar Clinical PathwaysŌäĀ Coordinator Goals ŌĆó Motivate Clients ŌĆō To become as independent as possible in monitoring and maintaining their own health status ŌĆó Provide Clients with the knowledge and skills ŌĆō To make informed decisions about their healthcare and quality of life ŌĆó Reduce negative outcomes ŌĆō Hospitalizations, Readmissions, Urgent Care Visits ,ER Visits, Falls, Med Errors, etc ŌĆó Maintain active communication ŌĆō BrightStar Clinical Pathway Team, ClientŌĆÖs Family and Physician, Other Healthcare Providers
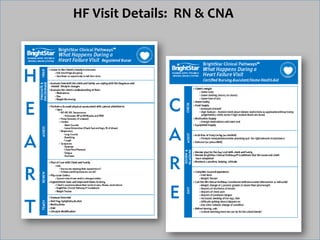
- 26. HF Visit Details: RN & CNA
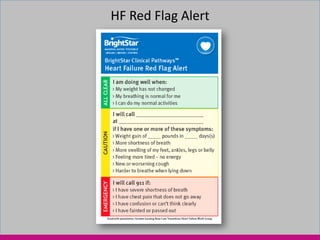
- 28. HF Red Flag Alert
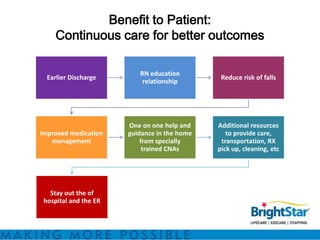
- 30. Benefit to Patient: Continuous care for better outcomes RN education Earlier Discharge Reduce risk of falls relationship One on one help and Additional resources Improved medication guidance in the home to provide care, management from specially transportation, RX trained CNAs pick up, cleaning, etc Stay out the of hospital and the ER
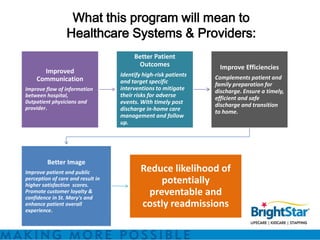
- 31. What this program will mean to Healthcare Systems & Providers: Better Patient Outcomes Improve Efficiencies Improved Identify high-risk patients Communication Complements patient and and target specific family preparation for Improve flow of information interventions to mitigate discharge. Ensure a timely, between hospital, their risks for adverse efficient and safe 0utpatient physicians and events. With timely post discharge and transition provider. discharge in-home care to home. management and follow up. Better Image Improve patient and public Reduce likelihood of perception of care and result in higher satisfaction scores. potentially Promote customer loyalty & confidence in St. Mary's and preventable and enhance patient overall costly readmissions experience.
- 32. Why BrightStar? Our Difference: ’ā╝ Joint Commission Accreditation ’ā╝ Commitment to RN oversight ’ā╝ Fully Licensed by the ’ā╝ Person centered approach ’ā╝ Press Ganey satisfaction survey ’ā╝ CareTogether┬« ’ā╝ Licensed and insured for transport ’ā╝ Flexible & responsive ’ā╝ RN DON trains & competency tests ’ā╝ Highly qualified and specially trained staff all CNAs ’ā╝ Stringent screening and employment ’ā╝ All patients receive in-home risk practices assessment to help reduce falls ’ā╝ HANDS ’ā╝ Continuity of care and care collaboration ’ā╝ BrightStar Clinical Pathways ’ā╝ Ongoing services to maintain safety ’ā╝ Locally owned & operated and success
- 33. Ask Me How We Can Make More Possible For You! Kym.Guy@BrightStarCare.com 805.358.6022
Editor's Notes
- #2: .
- #3: President Obama proposed $320 billion in reductions to Medicare and Medicaid as part of his $3.8 trillion fiscal year 2013 federal budget proposal. The presidentŌĆÖs plan, which is similar to a proposal the White House released in September, calls for cutting Medicare by $268 billion and Medicaid by $52 billion over 10 years.
- #9: With the HANDS program BrightStar caregivers would provide timely assistance upon hospital discharge, maybe even transporting the patient to their place of residenceSo we will facilitate a safe and supportive environment before a Medicare home health agency has the ability to take over care management, We will serve as an additional link in care coordination. When MC agency and therapy com in ŌĆ”collaborate with them supporting and reinforcing their teaching with the pt. - providing feedback , additional information they otherwise may not be able to obtain.- promoting even better outcomes than could have been possible before
- #14: ANDREW
- #15: it begins at the time of discharge and continues for a minimum of 4-weeks critical transition time for re-engagement in the home setting- matches the 30 readmission window associated with penalties
- #19: SHARON
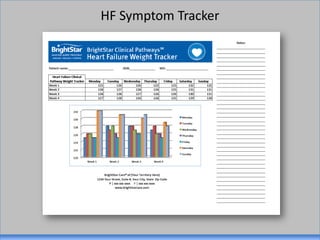
- #22: Example, Daily Weight CalendarŌĆ”
- #23: [explain Blue shows what Family schedules around the GREEN events that are those where BrightStar will be in the home]
- #27: DOUG
- #28: SHARON
- #29: SHARON
- #30: ANDREW
- #31: Family related/situation related/ afternoon evening dischargetimely visit by our RNCP Coord. Is the cornerstone of the program with safety assessment, med reconciliation, disease state education with attention to red flag symptoms.Person-centered services performed by our CNATransportation from hospital to home, Home Safety Check, Light Housekeeping, Retrieval of Simple Supplies (medications, groceries, etc), Light Meal Prep, following our Transition Check List which includes phone calls to loved ones, arranging/confirming follow-up appointment with discharging physician and so on ŌĆ”. Condition home may have been left inOut of the hospital -Until those unavoidable exacerbation of their chronic disease occurs
- #33: Our joint commission is firm evidence about the client care we provide. Both our accreditation and client satisfaction scores . At BS we have a wonderful asset in our PG reporting. We have an exclusive relationship with PG. our questions map those of HCAHPS and HHCAPSYou have a great deal of focus on client satisfaction and so do weSt BS we understand the importance of patient satisfaction-Our last PG survey revealed that 98% of our customers would refer us to family or friend.CareTogether. ŌĆō we know you have a similar program in Caring Bridge -ŌĆō Care Together is different and complementary. -The calendar/visit function and condition specific pt education materials that weŌĆÖve added to CareTogether really make it unique.┬Ā