
















BURNS assessment and management_GRP_1_PPT[1].pptx
- 1. BURNS IN CHILDREN PRESENTATED BY GROUP 1 9TH SEPTEMBER 2024
- 2. OBJECTIVES ? By the end of this presentation students should be able to: ? Define the term burns ? Describe the causes of burns in children ? Explain the pathophysiological changes of burn ? Outline the classification of burns according to depth, cause and severity
- 3. INTRODUCTION ?Burns are the second leading cause of accident deaths in childhood ?The highest incidence of burns occurs in children younger than 5 years. ?Children at high risk are those of lower social economic status and of single parent. ?However, any child, supervised or unsupervised, is at risk for a burn injury.
- 4. DEFINITION OF BURN ?Burn are the tissue injury caused by the contact with heat, frame, chemicals, electricity and radiation. ?The effect of burn injury are not limited to brunt area, but can cause serious systemic effect depending on the extent and depth of burn.
- 5. CAUSES OF BURN ? 1. scalds burn ? Burn injury caused by hot liquids (liquid hot food, hot water, tea, coffee milk) or stream. It is common in children below 3 year of age. ? 2. electric burn ? It is common in toddler and adolescents when playing with electrical outlet extension cord, touching, high tention wires, etc. ? 3. inhalation burn ? May occur from fire works
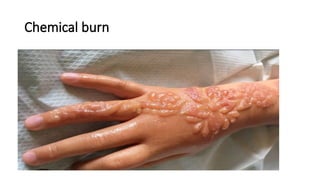
- 6. CAUSES OF BURN CNT.., ? Chemical burn ? Also common in children. Out of curiosity they handle household cleansing chemical, acids, etc. And they get injured. ? Open frame burn ? Common during playing with lighter or at kitchen near stove or over gas line. It may be happen from open fire in winter season or from fireworks during festivals our diwali.
- 8. SCALDS BURN RADIATION BURN
- 10. PATHOPHYSIOLOGY ? Burns cause immediate damage to the skin and underlying tissues, which may involve the epidermis, dermis, or even deeper tissues such as muscles and bones, depending on the burn depth (first, second, or third degree). ? The damaged tissues release inflammatory mediators such as histamines, prostaglandins, and cytokines, leading to vasodilation, increased capillary permeability, and edema formation. ? The loss of the protective skin barrier makes children susceptible to infections at the burn site.
- 11. PATHOPHYSIOLOGY CONT., ? Severe burns result in massive fluid loss due to the increased capillary permeability, leading to hypovolemia and the potential for hypovolemic shock. The loss of fluids can lead to electrolyte imbalances particularly hyponatremia and hyperkalemia which can have serious complications for cardiac function. ? Severe burns also lead to metabolic changes, thermoregulatory impairment, immune suppression and multi- organ dysfunction
- 12. PEDIATRIC CONSIDERATIONS ? Children have thinner skin than adults, which makes them more susceptible to deeper burns. They also have a proportionally lager body surface area relatively to their weight, which can result in greater fluid and heat loss. ? Additionally, their immature immune systems make them more vulnerable to infections and complications. ? Early and aggressive management, including fluid resuscitation, infection control, and nutritional support, is crucial in mitigating the pathophysiological changes and improving outcomes in pediatric burn patients.
- 13. CLASSIFICATION OF BURNS ? Burns can be classified based on their depth, cause, and severity. HereĪ»s a summary: ? 1. ACCORDING TO DEPTH ? A. First-Degree Burns (Superficial Burns) ? Affect only the outer layer of skin (epidermis).characterized by redness, minor swelling and pain. ? Example: Mild sunburn.
- 14. CNT., ? B. Second-Degree Burns (Partial Thickness Burns): ? Affect both the epidermis and part of the dermis. It is characterized by red blistered, swollen, and very painful; may appear shiny and wet ? Example: Scalds from hot liquids or severe sunburn. ? C. Third-Degree Burns (Full Thickness Burns) ? Involve the epidermis, dermis, and may extend into deeper tissue. It is characterized by white, charred, or leathery skin; may be painless due to nerve damage. Examples; flame burns or prolonged exposure to hot objects.
- 15. CNT., ? D. Fourth-Degree Burns ? Extend beyond the skin into underlying fat, muscle, or bone. ? Symptoms Blackened and charred appearance; often painless due to extensive nerve damage. ? Example: Severe electrical burns or prolonged flames.
- 16. 2. ACCORDING TO CAUSE ? A. Thermal Burns ? Causes: Hot liquids (scalds), flames, and contact with hot surfaces. ? B. Chemical Burns ? Causes: caustic substances like acids or alkalis. ? Example Household cleaners or industrial solvents. ? C. Electrical Burns ? Causes: Electrical currents passing through the body. Can cause deep tissue damage. ?
- 17. CNT., ? D. Radiation Burns ? Causes Sun exposure, radiation therapy, or other sources of radiation. ? E. Friction Burns ? Causes: Rubbing against a rough surface, commonly seen in road rash.
- 18. 3. ACCORDING TO SEVERITY (BASED ON SURFACE AREAAND DEPTH) ? Minor Burns ? - First-degree burns covering less than 10% of total body surface area (TBSA). ? - Second-degree burns covering less than 5% of TBSA. ? Moderate Burns ? - Second-degree burns covering 5-10% of TBSA. ? - Third-degree burns covering less than 5% of TBSA. ? Major Burns ? - Third-degree burns greater than 5% of TBSA. ? - Burns that involve critical areas (hands, face, feet, genitalia, or major joints) regardless of depth.
- 19. ?THANK YOU
- 20. REFERENCES ? Pattern of burns identified in the Pediatrics Emergency Department at King Abdul-Aziz Medical City: Riyadh ? Down loaden article http:// www.jsn brn.org retrived on Monday June 2016 ? Mariane et al (2005) Manual of Critical care Nursing fifth edition, USA