































More Related Content
What's hot (19)
Viewers also liked (6)



Similar to Cancer (20)




















Cancer
- 1. What is Cancer, anyway? A biological overview of the mechanisms of malignancy for computational and system biology researchers Pedro Romero, PhD. School of Informatics Center for Computational Biology and Bioinformatics Indiana University - Indianapolis
- 2. The “main source” The Biological Basis of Cancer Robert G. McKinnell, Ralph E. Parchment, Alan O. Perantoni, G. Barry Pierce 2nd. Ed. 2006 Cambridge University Press
- 3. Outline • The Pathology of cancer • The development of cancer • The stem cell model of tissue renewal • Stem cancer cell or cancer stem cell? • The Importance of a “Systemic” View
- 4. The Pathology of Cancer What is cancer and what it looks like
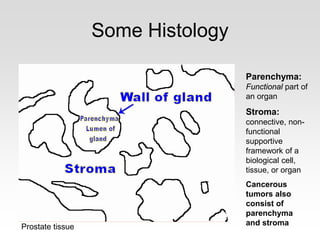
- 5. Some Histology Parenchyma: Functional part of an organ Stroma: connective, non- functional supportive framework of a biological cell, tissue, or organ Cancerous tumors also consist of parenchyma and stromaProstate tissue
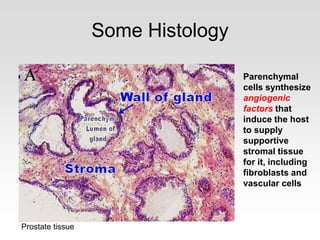
- 6. Some Histology Parenchymal cells synthesize angiogenic factors that induce the host to supply supportive stromal tissue for it, including fibroblasts and vascular cells Prostate tissue
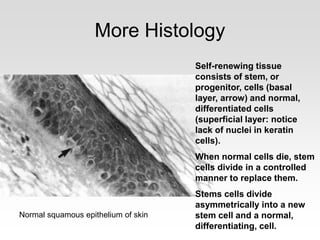
- 7. More Histology Self-renewing tissue consists of stem, or progenitor, cells (basal layer, arrow) and normal, differentiated cells (superficial layer: notice lack of nuclei in keratin cells). When normal cells die, stem cells divide in a controlled manner to replace them. Stems cells divide asymmetrically into a new stem cell and a normal, differentiating, cell. Normal squamous epithelium of skin
- 8. Altered states • Tissue changes: – Hyperplasia: Reversible tissue growth caused by environmental stimuli (e.g., hormones: Breasts enlarge during pregnancy and nursing) Cells grow in size and/or number. (Atrophy is the opposite effect) – Metaplasia: Reversible changes in differentiation caused by environmental stimuli (e.g., change from epithelial to squamous cells in lungs due to smoke) – Dysplasia: (Still) Reversible changes in normal maturation of cells due to persistent stimuli – cells differentiate poorly and can become malignant with prolonged exposure. – Neoplasia: Irreversible changes in cell proliferation and maturation that persist after the stimulus has disappeared. Neoplasms = Tumors (can be malignant). When restricted to one location and separated from stromal tissue, the neoplasm is said to be in situ (non invasive).
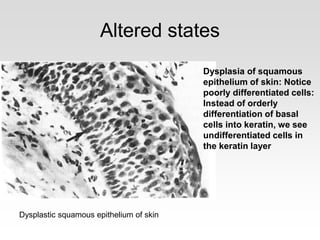
- 9. Altered states Dysplasia of squamous epithelium of skin: Notice poorly differentiated cells: Instead of orderly differentiation of basal cells into keratin, we see undifferentiated cells in the keratin layer Dysplastic squamous epithelium of skin
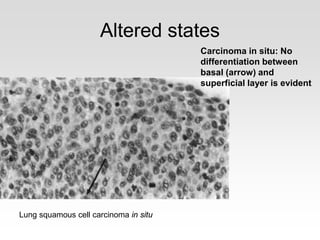
- 10. Altered states Carcinoma in situ: No differentiation between basal (arrow) and superficial layer is evident Lung squamous cell carcinoma in situ
- 11. Tumors: Good and Bad • Benign tumors: – Slow growing neoplasms – Designated by tissue + suffix -oma – Well differentiated cells (rare cell division) – Similar to normal tissue – Secretes same proteins, but can do so in uncontrolled fashion – Excessive growth can push and compromise adjacent tissue
- 12. Tumors: Good and Bad • Malignant tumors: – Neoplasms with malignant tendencies: • Uncontrolled growth • Invasion of normal tissue • Metastasis → Host death – Malignant cells: • Pleomorphic (varied size/shape) • Anaplastic (undifferentiated) • Atypical nuclei / High nucleus-cytoplasm ratio • Can also excrete proteins and other molecules as normal tissue → Potential tumor markers
- 13. Tumors: Good and Bad • Malignant tumors nomenclature (suffixes): – Epithelial: -carcinoma, – Mesenchymal (bone, fat, cartilage): -sarcoma – Embrionic/Child: -blastoma – Other: • Glioma (brain) • Lymphoma (lymphocytes, always malignant) • Seminoma (germ cells) • Skin pigmented cells or melanocytes (melanoma) • Leukemias
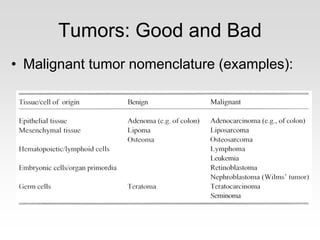
- 14. Tumors: Good and Bad • Malignant tumor nomenclature (examples):
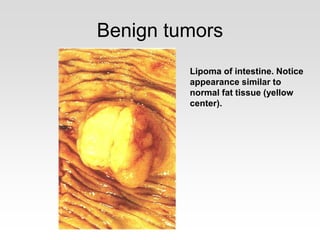
- 15. Benign tumors Lipoma of intestine. Notice appearance similar to normal fat tissue (yellow center).
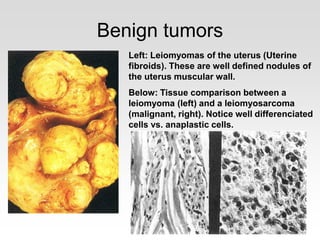
- 16. Benign tumors Left: Leiomyomas of the uterus (Uterine fibroids). These are well defined nodules of the uterus muscular wall. Below: Tissue comparison between a leiomyoma (left) and a leiomyosarcoma (malignant, right). Notice well differenciated cells vs. anaplastic cells.
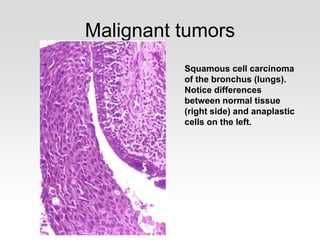
- 17. Malignant tumors Squamous cell carcinoma of the bronchus (lungs). Notice differences between normal tissue (right side) and anaplastic cells on the left.
- 18. Tumor staging Overall Stage Grouping is also referred to as Roman Numeral Staging. This system uses numerals I, II, III, and IV (plus the 0) to describe the progression of cancer. • Stage 0 carcinoma in situ. • Stage I cancers are localized to one part of the body. • Stage II cancers are locally advanced, as are Stage III cancers. Whether a cancer is designated as Stage II or Stage III can depend on the specific type of cancer. • Stage IV cancers have often metastasized, or spread to other organs or throughout the body. • A cancer may also be designated as recurrent, meaning that it has appeared again after being in remission or after all visible tumor has been eliminated. Recurrence can either be local, meaning that it appears in the same location as the original, or distant, meaning that it appears in a different part of the body.
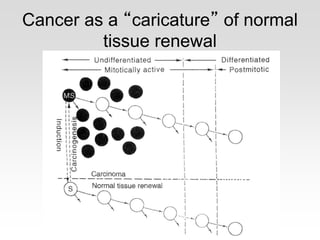
- 19. Cancer as a “caricature” of normal tissue renewal
- 20. The Development of Cancer From carcinogenesis to metastasis: The dangerous life and evolution of “bad” cells
- 21. The processes of cancer • Carcinogenesis – Initiation: Carcinogen modifies DNA – Latency: Period between initiation and tumor formation. Need appropriate environment (promoters) to express phenotype – Promotion: Application of promoters and other environmental factors leads to tumor formation. Tumors regress when promoters are removed. – Progression: Evolution towards autonomous stage (independence from environmental factors) – Conversion: Malignant neoplastic phenotype • Metastasis • Malignant cell dissemination. Requires autonomous cells with special abilities (i.e., converted cells)
- 23. Initiation • Chemical carcinogenesis – Carcinogens usually interact with DNA and generate “adducts” that cause copy errors – Some carcinogens act directly, some have to be metabolized first into an “active” form – Not all carcinogens are mutagenic, and not all mutagenic substances are carcinogenic – Exogenous • Man-made • Naturally occurring – Endogenous • Free radicals
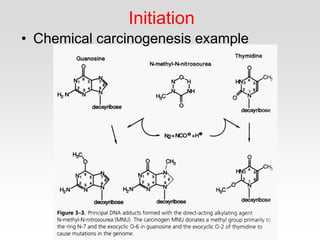
- 24. Initiation • Chemical carcinogenesis example
- 25. Promotion • Promoters are usually not genotoxic, as opposed to carcinogens • Promotion seems to be an epigenetic process related to gene expression and regulation • Promoters believed to stimulate growth and prevent apoptosis / differentiation in initiated cells • Promoter presence induces proliferation of initiated cells into tumors • Withdrawal of promoter at this stage results in complete regression of these lesions
- 26. Promotion • Chemical promoters – Exogenous – Endogenous (hormones, growth factors) • Promotion processes – Hyperplasia (selective proliferation) – Reduction of tissue regulation on initiated cell • Cytotoxicity (kill surrounding normal cells) • Inhibition of inter-cellular communication – Cytotoxicity also promotes growth factor activity needed for cell repair, which helps proliferation
- 27. Progression • Progression enhances aggressiveness of tumor cells and lead to autonomous cells through different routes: – Defects in apoptosis – Increase in proliferative cell population – Decrease of tendency to terminally differentiate – Shift towards autonomous growth – Genetic instability – Invasive metastatic behaviors • Cells show great heterogeneity, which is gradually reduced through selection
- 28. Conversion • At the end of the progression phase, cells have converted to the malignant phenotype – Invasive – Highly autonomous – Can erode tissue barriers – Can escape both physical and regulatory constraints from surrounding normal tissue
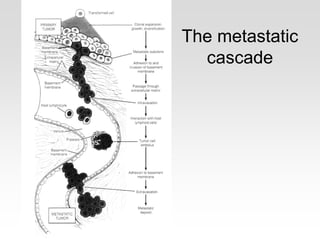
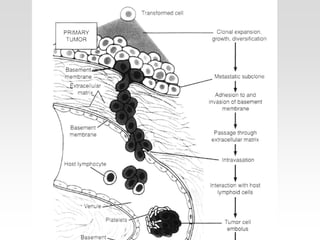
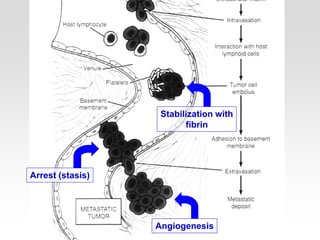
- 29. Metastasis • The metastatic cascade – Disruption of basal membrane – Cell detachment (separation) – Cell motility – Invasion – Penetration of vascular system – Circulating cancer cells – Arrest (stasis) – Extravasion and proloferation
- 32. Disruption of basal membrane and stroma invasion • Basal membrane separates epithelium from stromal extracellular matrix (ECM) • Controlled enzymatic digestion of ECM components is a major step in metastasis – Type IV collagen-degrading enzymes for basal membrane – Type I collagenase for stromal tissue – Other proteolytic enzymes for digestion of fibronectin, elastin, proteoglycans, among others – Matrix metalloproteinases (MMP) can degrade any proteins in the ECM. Elevated MMP activity always found in malignant tissue – Cathepsins hydrolize peptide bonds – Enzyme inhibitors are promising anti-metastatic agents
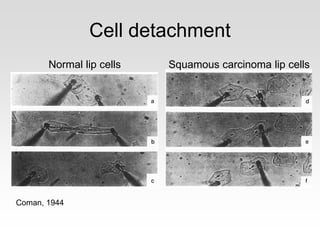
- 33. Cell detachment • Reduced cohesion is essential • Expression of E-cadherin is essential for conservation of normal epithelial morphology and non-invasive phenotype • Lack of E-cadherin produces loss of morphology and invasiveness • Transfection of malignant cells with E- cadherin cDNA blocks invasion • Detachment is critical for metastasis
- 34. Cell detachment Coman, 1944 Normal lip cells Squamous carcinoma lip cells
- 35. Cell Motility • “Amoeboid” motility of cancer cells first reported by Virchow in 1863. Confirmed in vitro in 1939 and 1950, and in vivo in 1998 • Cells have to migrate individually • Embryonic cells also have the ability to migrate • Autocrine motility factor (AMF) and its receptor (AMF-R) stimulate motility. Their expression in malignant tissue correlates with aggressiveness • The tubulin-based cytoplasmic microtubule complex (CMTC) is implicated in directional migration • Agents that depolymerize microtubules inhibit invasion (vinca alkaloids and nocodazole)
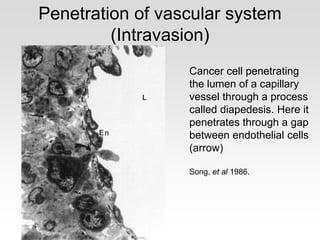
- 36. Penetration of vascular system (Intravasion) • Invading cells move towards capillaries and lymphatic vessels in ECM with the help of digestion enzymes • Density of capillaries in a tumor is positively correlated with metastatic behavior • Newly formed blood vessels have small defects (gaps and membrane discontinuities) • Type IV collagenase helps breach capillary membranes • Most cells are damaged or destroyed upon entrance to the circulation
- 37. Penetration of vascular system (Intravasion) Cancer cell penetrating the lumen of a capillary vessel through a process called diapedesis. Here it penetrates through a gap between endothelial cells (arrow) Song, et al 1986.
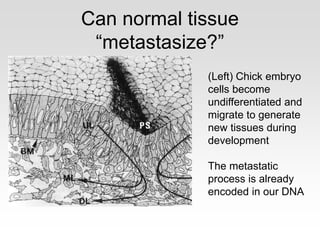
- 39. Can normal tissue “metastasize?” (Left) Chick embryo cells become undifferentiated and migrate to generate new tissues during development The metastatic process is already encoded in our DNA
- 40. The Stem Cell Model of Tissue Renewal Avenues for potential therapies
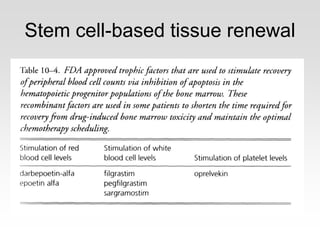
- 41. Stem cell-based tissue renewal
- 42. Stem cell-based tissue renewal
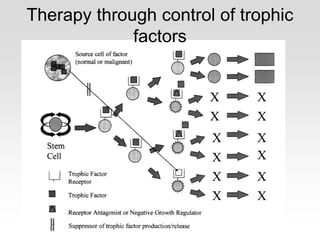
- 43. Therapy through control of trophic factors
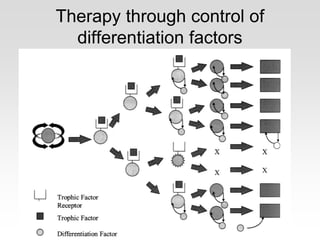
- 44. Therapy through control of differentiation factors
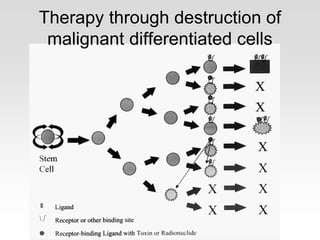
- 45. Therapy through destruction of malignant differentiated cells
- 46. Stem cancer cell or cancer stem cell? Well… both!
- 47. Cancer vs stem cell
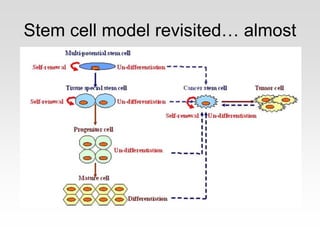
- 49. Stem cell model revisited… almost
- 50. The Importance of a “Systemic” View Parting Thoughts
- 51. Cancer is a natural selection process • Cancer is based on mutations, but not those which generate new abilities, but mainly those which access potential abilities • Many of these abilities are expressed in embryonic cells during early development • Mutations allow for selectively turning “on” and “off” specific processes. • Genes involved are oncogenes and tumor supressor genes
- 52. Understanding cancer provides “systemic” view • Framework for molecular studies of cancer – Oncogenes – Cancer related pathways • Metabolic • Regulatory • Signaling – Cancer related protein interactions – Put all these in relation to the cancer process as a whole – Do not just target genes or pathways: attack processes or at least be aware of them!
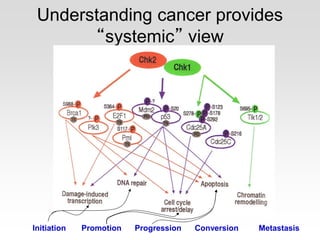
- 53. Understanding cancer provides “systemic” view Initiation Promotion Progression Conversion Metastasis
- 54. THANKS!