



























CANCER OF LARYNX AND ITS DETAILED MANAGEMENT
- 1. CANCER LARYNX SUBMITTED BY SATHEAHWARI N MSC N II YR
- 2. INTRODUCTION ŌĆó Cancer of the larynx is a malignant tumour in and around the larynx (voice box). Squamous centre carcinoma is the most common form of cancer of the larynx (95%). ŌĆó Cancer of the larynx occurs more frequently in men than in women, and it is most common in people between the ages of 50 to 70 years of age. ŌĆó It accounts for approximately half of all head and neck cancers. Almost of all malignant tumours of the larynx arise from the surface epithelium and are classified as squamous cell carcinoma.
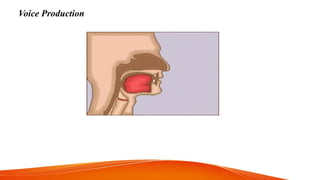
- 3. LARYNX ŌĆó It is an organ that provides a protective sphincter at the inlet of the air passage and is responsible for voice production. ŌĆó It extends from the tongue to the trachea (from the level of the upper border of the epiglottis to the level of the 6th vertebra).
- 4. RELATIONS ŌĆó Above :- Continous with pharynx ŌĆó Below :- Continous with trachea ŌĆó Anteriorly :- Covered by skin, superficial facia, deep fascia and infrahyoid muscles. ŌĆó On each side :- to the thyroid lobe.
- 5. STRUCTURE
- 6. CARTILAGE FRAMEWORK OF THE LARYNX ŌĆó Three large unpaired cartilages 1. Thyroid 2. Cricoid 3. Epiglotis ŌĆó Three small paired ŌĆó cartilages 1. Arytenoid 2. Corniculate 3. Cuneiform
- 7. FUNCTIONS OF LARYNX ŌĆó Maintain an open passageway for air movement (thyroid and cricoid cartilages) ŌĆó Epiglottis and vestibular folds prevent swallowed material from moving into larynx. ŌĆó vocal folds are primary source of sound production. Greater amplitude of vibration. ŌĆó The Pseudostratified ciliated columnar epithelium traps debris, preventing their entry into the lower respiratory tract. ŌĆó Respiration ŌĆó fixation of chest ŌĆó Helps in promoting venous return
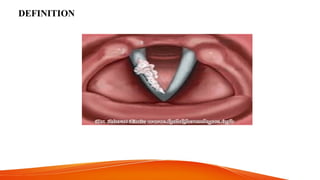
- 9. DEFINITION
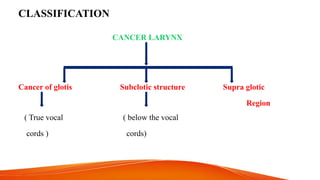
- 10. CLASSIFICATION CANCER LARYNX Cancer of glotis Subclotic structure Supra glotic Region ( True vocal ( below the vocal cords ) cords)
- 12. CAUSES AND RISK FACTORS
- 13. PATHOPHYSIOLOGY
- 14. CLINICAL MANIFESTATIONS ’üČ Depends on the site of tumour Glotic tumour voice changes Hemoptys is Dyspepsia pain weight loss respirator y obstructio n dyspnea
- 15. SUPRAGLOTIC TUMOUR ŌĆó Aspiration on swallowing ŌĆó Sore throat ŌĆó Foreign body sensation ŌĆó Dysphagia ŌĆó Neck mass ŌĆó Dyspnoea ŌĆó Pain in the throat referred to the ear
- 16. SUBGLOTTIC ŌĆó Airway obstruction ŌĆó Dysphagia ŌĆó Weight loss ŌĆó Hemoptysis
- 17. OTHER SYMPTOMS ’ā╝ Hoarseness of voice ’ā╝ Persistent cough ’ā╝ Sore throat ’ā╝ Throat pain ’ā╝ Throat burning (when consuming hot liquids or citrus fruits juices) ’ā╝ Lump felt in the neck ’ā╝ Dysphagia ’ā╝ Dyspnoea ’ā╝ Unilateral nasal obstruction ’ā╝ Nasal discharge ’ā╝ Foul breathing
- 19. MANAGEMENT ŌĆó MEDICAL MANAGEMENT Chemotherapy - For patients with more advanced disease - Cisplatin based chemo with radiation is used. - 5 fluorouracil also used
- 20. Radiation therapy - Goal of radiation is destroy cancer cells and preserve the function of the larynx - It can be used pre operatively and post operatively - It is combined with surgery in advanced conditions as adjuvant therapy.
- 21. SURGICAL MANAGEMENT Vocal cord strapping ŌĆó Stripping of vocal cord is used to treat dysphagia, hyperkerotosis and leukoplagia. ŌĆó the procedure involves removal of the mucosa of the edge of the vocal cord, is by using an operating microscope.
- 22. Cordectomy surgical removal of the vocal cord, is usually performed via transoral laser. Laser surgery When the tumour size is of small tumour are eradicated with the used of user. Microelectrodes of small tumours of the lungs. Partial laryngectomy A partial laryngectomy is often used smaller cancers of larynx. It is recommended in the early stage of cancer in the glottis area when only one vocal cord is involved. In this portion is removed along with the vocal cord and the tumour, all other structure remain.
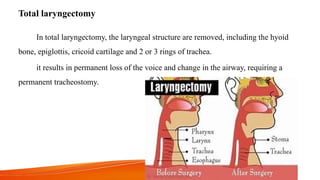
- 23. Total laryngectomy In total laryngectomy, the laryngeal structure are removed, including the hyoid bone, epiglottis, cricoid cartilage and 2 or 3 rings of trachea. it results in permanent loss of the voice and change in the airway, requiring a permanent tracheostomy.
- 24. NURSING MANAGEMENT PRE-OPERATIVE 1. Risk of aspiration related to cancer larynx and excessive secretions 2. Ineffective airway clearance related to increased tracheo branchial secretions 3. Risk of impaired gas exchange related to airway blockage secondary to tumour 4. Imblanced nutrition less than body requirement related to dysphagia
- 25. Post operative 1. Acute pain related to surgical incision 2. Ineffective airway pattern related to tracheo branchial secretions 3. Fluid volume deficit related to nil per ora status 4. Imbalanced nutrition less than body requirement related to less oral intake 5. ineffective communication pattern related to surgical removal of vocal cord and loss of voice. 6. Risk for aspiration related to surgical procedure
- 26. 1. Anxiety related to diagnosis ( disease condition and surgery) 2. Deficit knowledge about surgical procedure 3. Body image disturbance related to surgical corrections and tracheostomy 4. Self care deficit related to pain and weakness
- 27. SWALLOWING TECHNIQUE AFTER A PARTIAL LARYNGECTOMY ŌĆó Being with soft or semi solid foods. ŌĆó Stay with a nurse or swallowing therapist during meals until you master the technique of swallowing without choking. ŌĆó Be patient, learning to swallow again frustrating. ŌĆó Follow these steps in squence Take a deep breathe Bear down to close the vocal cords Place food into your mouth
- 28. Swallow Cough to rid the closed cord of accumulated food particles Swallow cough Breathe
- 29. NURSING CARE AFTER LARYNGECTOMY ŌĆó NUTRITION 1. Immediately after surgery, the clientŌĆÖs nutrition is supplemented with tube feedings. 2. The client contious to receive tube feedings until edema has subcided and suture line healing ha occured. 3. When the client can swallow saliva, oral feedings can begin. 4. The client usually begins with liquid or semi-solid foods and progresses as healing occurs.
- 30. ŌĆó COMMUNICATION 1. For the first days after surgery, the client should communicate by writing. 2. Even though cannot speak, conversation should still include the clientŌĆÖs input through noddding and pointing and not to be directed only to others, such as the family. 3. Avoiding conversation or excessive talking with client because of difficulty in communication is demeaning to the client and leads to frustration.
- 31. ARTIFICIAL LARYNX ŌĆó An artificial larynx may be used asearly 3 to 4 days after surgery. ŌĆó These battery operated speech devices are held alongside the neck or can be adapted with a plastic tube that is inserted with a plastic tube that is inserted into the mouth. ŌĆó The air inside the mouth is vibrated and the client articulates as usual. ŌĆó The speech quality is monitone amd mechanical soulding but intelligeible.
- 32. image
- 33. ESOPHAGEAL SPEECH ŌĆó Esophageal speech is a technique that requires the client to swallow and hold the air in the upper esophagus. ŌĆó By Controlling the flow of air, the client cannpronounce as many as 6 to 10 words before stopping to allow more air. ŌĆó The voice is deep but is one and effective the technique is mastered.
- 34. TRACHEO ESOPHAGEAL PUNCTURE ŌĆó It is a technique that also restores speech. A small puncture is made into upper tracheo stoma to the cervical esophagus for creation of a fistula. ŌĆó After fistula tract has healed, a small one way valve, or voice prosthesis is inserted. ŌĆó By occlusion of the prothesis, air can be stunted into the esophagus and used to produce speech. The TEP may be done concurrently with total laryngectomy.
- 35. SPEECH THERAPY ŌĆó To plan post operative communication strageiesnand speech therapy, the speech therapist or pathologist conduct a pre- operative evaluation. ŌĆó During this time, the nurse discussess with the patient and family about methods of communication that will be available in the immediate post- operative period. ŌĆó These include writing, lip, speaking and reading and communication or word boards. ŌĆó In addition, a long term post perative communication plan for a laryngeal communiction is developed. ŌĆó The inpatient common techniques of alaryngeal communication are elcetrodes esophageal speech and tracheo esophageal puncture.
- 36. COMPLICATIONS ŌĆó Respiratory distress ( hypoxia, airway obstruction) ŌĆó Haemorrhage ŌĆó Infection ŌĆó Wound breakdown ŌĆó Aspiration ŌĆó Dehydration