Carcinogenesis and mechanism of cancer -.pptx
•Download as PPTX, PDF•
0 likes•23 views

Cancer carcinogenesis






























Carcinogenesis and mechanism of cancer -.pptx
- 1. BSc Nursing.(Basic) MEDICAL Surgical Nursing Unit-VI. Oncology Nursing Carcinogensis, Early detection &Prevention Prof.P.Kuzhanthaivel Dept of Medical surgical Nursing
- 2. INTRODUCTION • Cancer refers to a large group od disorders with different manifestations ,treatment s and prognoses. It involves different organs and systems.
- 3. DEFINITION OF TERMS • Cancer is a group of diseases involving abnormal cell growth with the potential to invade or spread to other parts of the body. These contrast with benign tumors, which do not spread. • Carcinogensis -The process by which normal cells are transformed into cancer or malignant cells. • Tumor- Abnormal cell growth leading to new cell mass that has no functional purpose. • Benign Tumor- New growth of cell mass that not spread to other organs. less aggressive , less life threatening. • Malignant tumor- Life threatening abnormal cell growthwhich grows and spreads rapidly is called malignant tumor. It is otherwise known as cancer.
- 4. ETIOLOGY 1. GENETIC AND FAMILY HISTORY 2. VIRUSES AND BACTERIA 3. PHYSICAL AGENT 4. CHEMICAL AGENT 5. DIETARY FACTORS 6. HORMONAL AGENTS 7. ROLE OF THE IMMUNE SYSTEM
- 5. GENETIC AND FAMILY HISTORY Almost every cancer type has been shown to run in families Genetic factor play a role in cancer cell development Abnormal chromosomal patterns and cancer have been associated with extra chromosomes or translocated chromosomes 5 to 10% caused by genetic and family history Cancer breast is found in first degree relatives. Autosomal dominant factors are found in cancer breast, cancer ovary,retinoblastoma, wilms tumour, prostate cancer etc
- 6. VIRUSES AND BACTERIA • 11% of all cancers worldwide are linked to viral infection • Viruses can cause cancer by two ways- 1) After infecting individuals DNA viruses insert a part of their own DNA near the infected cell genes causing cell division 2) The newly formed cells that now carry viral DNA lack normal control on growth Example of viruses that causes cancer: Human Pappiloma Virus- Cancer cervix, head and neck cancers, Heptitis B virus - Hepatic carcinoma, Epsein Barr Virus- Butkitts lymphoma. Bacteria: H. pylori is a one of the bacterium cause gastric malignancy
- 7. PHYSICAL AGENTS • Exposure to sunlight or radiation • Exposure to UV rays of the sun cause skin cancer • Exposure to ionising radiations can occur with repeated diagnostic X-ray procedures cause cancer • Radiation therapy used to cancer treatment and exposure to radioactive materials at nuclear weapon manufacturing sites • .Nuclear power plants produce high incidence of leukaemia, multiple myeloma, and cancer of lung, bone, breast and thyroid
- 8. CHEMICAL AGENTS • Most hazardous chemicals produce the toxic effects by altering DNA structure in body sites • Tobacco smoke accounts for 30% of cancer death in humans • More than 4000 chemicals have been identified in tobacco smoke and in that more than 60 chemicals are carcinogens • Chemicals include aromatic amines & aniline dyes pesticides, formaldehydes, arsenic, soot & tars asbestos, benzene, betel and nut, cadmium, chromium compounds, nickel and zinc ores, wood dust, beryllium compounds and polyvinyl chloride cause cancers
- 9. DIETARY FACTORS • Dietary substances that appear to increase the risk of cancer include fat, alcohol , salt-cured or smoked meats, nitrate and nitrite containing foods, red and processed meats • Poor diet and obesity have been identified as contributing factors for the development of cancers • Chronic severe malnutrition is implicated for cancer in postmenopausal women
- 10. HORMONAL AGENTS • Tumour growth may be promoted by disturbance in hormonal balance • Ca breast, Ca prostate and Ca uterus are thought to be depends on endogenous hormonal levels for growth • Diethylstilbesterol (DES) has been recognised as a cause of vaginal carcinoma • Oral contraceptives and prolonged estrogen therapy are associated with an increased incidence of hepatocellular, endometrial and breast cancers
- 11. ROLE OF THE IMMUNE SYSTEM • The immune system recognizes the Tumour Associated Antigen (TAA) . The macrophages and dentritic cells identify and present it of T lymphocytes and kills by 3 mechanisms 1.T lymphocytes secretes cytokines that kills the tumour cells in very early stage itself. 2.Induce apotosis (Cell death)of tumour cells 3. T -cytotoxic cells are induces which kills tumour cells • Sometimes Immune system fails to identify and stop the growth of transformed cells, cancer develops • Patient who are immuno-compromised have an increased incidence of cancer
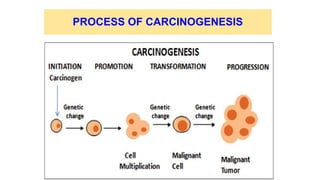
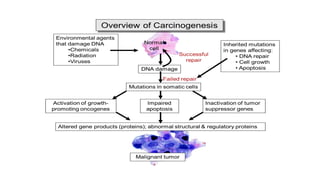
- 15. INITIATION PHASE • Agents that initiate cellular transformations are referred to as carcinogens • During initiation, carcinogens such as chemicals, physical factors, biologic agent cause mutations in the cellular DNA • Normally, the alterations are reversed by DNA repair mechanisms or programmed cell death (apoptosis)
- 16. PROMOTION PHASE • During promotion, repeated exposure to promoting agents (co- carcinogens) causes proliferation and expansion of initiated cells with increased manifestation of abnormal genetic information even after long latency period • Latency periods for the promotion of cellular mutation vary with type of agent, the dosage of promoters, and the innate characteristics and genetic stability of the target cell • Promotion phase generally leads to the formation of pre-neoplastic lesion or benign lesion
- 17. TRANSFORMATION & PROGRESSION PHASE • Transformation phase - During transformation phase, multiplied cells will become malignant cells • Progression phase -During progression, the altered cell exhibit malignant behaviour. Malignant cells acquire the ability to stimulate angiogenesis to invade adjacent tissues and to metastasis
- 18. THEORIES OF CARCINOGENESIS 1. GENETIC THEORY 2. EPIGENETIC THEORY 3. IMMUNE SURVEILLANCE THEORY 4. MONOCLONAL HYPOTHESIS 5. MULTI – STEP THEORY
- 19. THEORIES OF CARCINOGENESIS • Genetic theory - Popular theory .cell become neoplastic because of alteration in the DNA. The mutated cells transmit their characteristics to the next progeny cells. • Epigenetic theory-The carcinogenic agents act on activators or suppressors of genes and not on the genes themselves and result in the abnormal expression of the genes. • Immune surveillance theory- An immune – competent host mounts an attack on developing tumor cells so as to destroy them while an immune – competent host fails to do so.
- 20. THEORIES OF CARCINOGENESIS contd • Monoclonal hypothesis evidence on studies of human and experimental tumors that most cancers arise From A Single clone of transformed cells. • Multi – step theory -According to this theory oncogenesis is a multi – step process namely 1. Initiation 2. Promotion 3.Progrssion
- 22. HALLMARKS OF CANCER 1. Unregulated cell growth . 2. Cells do not obey the natural cell death call (Apoptosis)given by the body’s immune system 3. Cells have multiple configuration or morphological changes. 4. It develops aggressive growth into adjacent structures, blood vessels and lymphatic cells and destroy those cells .There by it invade the blood stream/lymphatics and spread to distant tissues. Lymph glands. 5. Develop new blood vessels in the tumour mass.
- 24. HALL MARKS OF CANCER CELLS 1.Growth promoting oncogenes-Mutated form of normal proto- oncogenes in cancer is called oncogenes - Mutation in the structure of genes -Lacking the normal growth promoting signals of proto-oncogenes -They act by over expression to promote autonomous and excessive cell proliferation by GFs,GF Receptors,signal transduction proteins(RAS genes) 2.Growth suppressing antioncogenes-Mutated Anti-Oncogene behave like growth promoting oncogenes.Eg.BRCA1 & BRCA 2 Genes
- 25. HALL MARKS OF CANCER CELLS contd • 3.Genes regulating apoptosis & cancer-In cancer cells, the function of apoptosis is interfered due to mutation in growth promoting oncogenes which regulate apoptosis in normal cells. Here tumor growth is by escaping apoptosis. • Eg.CD95 receptors are depleted in hepatocellular carcinoma & hence the tumor cell escape from apoptosis.
- 26. HALL MARKS OF CANCER CELLS contd 4.Telomeres & telomerase in cancer • Telomeres: There is progressive shortening of telomeres which are terminal tips of chromosomes. • Telomerase:It is the RNA enzyme that help in repair in DNA & maintain normal telomere length.It is active in normal stem cells but not in normal somatic cells. • Avoid cellular aging,mitosis does not slow down or cease,thereby proliferation of cancer cells occur. 5.Tumor Angiogenesis - Cancer can survive if the cancer cells are adequately nourished and perfused . Continued perfusion of cancer occur by vascular endothelial growth factors
- 27. HALL MARKS OF CANCER CELLS contd 6.Cancer dissemination -Invasion and distant metastasis occur 7.Mutator genes & cancer-DNA repair is defective as happens in some inherited mutation & the defect in DNA is passed to the next progeny of cells and cancer results. Eg.Hereditory non-polyposis colon cancer • 8.Clonal aggressiveness -Cancer progression are increasing size of the tumor,higher histologic grade,areas of tumor necrosis and invasiveness & distant metastasis.
- 28. DIFFERENCE BETWEEN BENIGN AND MALIGNANT TUMOR Benign Tumor • Cells – Well differentiated, resembles the normal cells of origin from where tumor grows • Mode of growth-Grows by expansion and does not invade the adjacent structures. • Rate of growth is usually slow. Malignant tumor • Cells – Undifferentiated and have little resemblence of normal cells from where the tumour originated. • Mode of growth- Grow by local infiltration and invasion and overcome contact inhibition. • Rate of growth varies with degree of differentiation. More anaplastic the more rapid it grows.
- 29. Difference between Benign and Malignant tumour contd Benign Tumour • Metastasis-No distant metastasis • Shape – Usually encapsulated and regular cell mass • General effects - Usually less serious, cause a local phenomenon. Only when it is located in crucial place can cause serious effects • Does not usually cause death Malignant tumour • MetastasisSpread by distant metastasis by gaining entry into blood vessels or lymphatic channels • Shape-Irregular margins and is not encapsulated • General effects-Produce systemic impacts, anemia, weakness, systemic inflammations, weight loss, and cachexia • Eventually cause death unless growth is controlled.
- 30. DIAGNOSIS & EARLY DETECTION • History of functional and structural changes such as new mass , abnormal discharges, abnormal cough, voice etc. Detect for CAUTION • C-Changes in bowel or bladder habits • A- Any unhealed ulcer • U –Unusal bleeding or discharges • T- Thickening or lump anywhere in the body • I- Indigestion or inability to swallow • O- Overt changes in the wart or mole • N- Nagging cough or horseness of voice
- 31. EARLY DETECTION • Ca. Breast- Mammography, Ultrasound for women of the age 45-54, • Ca.Cervix- PAP smear test every three years and later every five years for women after 21 who are sexually active • Colorectal cancer-Men and women of age 50 +stool test for occult blood • Ca. Prostate-Digital rectal examination and prostate specific antigen. • Testicular self examination and clinical testicular examination for detection of Ca. testes.
- 32. COMMON DIAGNOSTIC TEST • Blood test • Cancer specific antigens • Ultrasound • X-ray Studies • Barium Studies • Upper and lower GI scopies • Hysterosaplhingscope • Bronchoscopies • MRI • CT and PET scan
- 33. CONFIRMATORY TESTS • Biopsy – Which can be open or fluoroscopy guided biopsy or • FNAC-Fine needle aspiration Cytology • PET scan – Confirms the extent of metastasis
- 34. STAGING TNM CLASSIFICATION • TNM Classification • T-Tumor size at the primary site • N- Nodal involvement • M- Presence of metastasis PRIMARY TUMUR SIZE (T) • Tx-Primary tumor size cannot be assessed • To- No evidence of primary tumur • Tis- Tumur In situ • T1 , T2, T3 T4- Increasing size of the primary tumur.
- 35. GRADING OF CANCER Pathological classification of cancer is called Grading . It is very useful diagnostic tool . Based on grading the treatment decision is made. It is a good prognostic indicator. Grade I-Well differentiated tumor cells closely resemble the tissue of structure and function. Grade II- Intermediate differentiation and grow faster than normal tissue Grade III-Poorly differentiated with less resemblance of the tissue of origin Grade IV- Undifferentiated tumor cells , higher level of abnormality in structure and function.
- 36. PREVENTION • Prevention of obesity and Maintaining ideal BMI • Engage in regular physical activity • Limit processed meat and red meat • Choose whole grains, instead of processed refined grains or flours. • Vegetables such as cauliflower, broccoli, cabbage etc having substances that prevent promotion of cancer • Eating lugumes, nuts, fresh fruits and leafy vegatbles are found to be helpful • Avoid constipation
- 37. PREVENTION contd • Abstinence from alcohol or limiting is and • smoking cessation • Applying personal protective equipment while at work in industrial sector that emits high level of carcinogenic chemicals (Eg-benzene, formaldehyde, arsenic, tar,asbestos,cadmium Polyvinyl chloride.) • Vaccination- Heptitis B vaccine can prevent liver cancer • HPV vaccination( Gardacil ) is recommended for prevention of Ca. Cervix.
- 38. References • Sharma.S.K., Madhavi.S.Hinkle.J.,& Cheever.K.- Brunner& Suddharth Text book of Medical Surgical nursing 2018, 1st SAE, New delhi, Wolters Kluwer. • Lewis-Medical Surgical Nursing 2009,Elsevier • Sherly otto- Text book of Oncology nursing • Robinson-text book of Pathology • Davidson’s Principles and Practice of medicine,2010,Elsevier