































CAse presentation on pediatric hydrocephalus
- 1. CASE PRESENTATION By Dr. Saifullah Chang House Officer Pediatric department GMMMC
- 2. HISTORY: ’éó 21 days Abdul Kabeer S/O Shahnawaz Muhammad Naveed R/O Sukkur , vaccinated according to EPI schedule; presented to us with complain of ’éó Fits ’éó Fever 5th day of life
- 3. HOPI: ’éó Fits were sudden in onset just after birth, generalized tonic clonic in nature with up rolling of eyes , continued for 6 hours in duration, multiple attacks with interval of 15 minutes apart ’éó Baby taken to private hospital , went under treatment and discharged on tab. Pheno ’éó Then developed fits and fever at 5th DOL ’éó Fits were of same nature ’éó Fever was sudden in onset, high grade ,not associated with rigors and chills or respiratory distress , relieved by injectable medications given at peads emergency
- 5. ANTENATAL: ’éó Mother was young aged approx. 18 years with good nutritional status and healthy background ’éó No any history of chronic maternal illness ’éó Booked case ’éó Vaccinated for tetanus ’éó Multivitamin supplements during pregnancy ’éó 5 U/S were done at 3rd 6th 7th 9th months respectively all were normal showing single intrauterine fetus with adequate growth , cardiac activity and liquor ’éó No history of leaking and P/V bleeding ’éó No any adverse previous obstetric outcome
- 6. NATAL: ’éó History of prolonged labour one hour in duration ’éó Trial taken by dia at home ’éó Emergency cesarean section was done at local private setup
- 7. POST NATAL: ’éó History of delayed cry, after one hour of birth ’éó Suctioning and tactile stimulation was done ’éó Resuscitation was done in OT ’éó Baby developed fits after then ’éó Incubated for 4 days at private setup ’éó No history of jaundice and skin rash
- 8. FEEDING HISTORY: ’éó Breastfed at 5th D.O.L ’éó No any history of early introduction of enteral feed
- 9. FAMILY HISTORY: ’éó First baby ’éó no previous issue ’éó History of child with cerebral palsy in paternal side of family
- 10. ON EXAMINATION: An ill pale looking lethargic baby, on oxygen support through nasal cannula , cannulated on left foot , lying on bed poorly responsive to tactile stimulation , not crying well Vitals ŌĆó HR:128 B/P/M ŌĆó RR:46 B/min ŌĆó Temp:99.8F ŌĆó FOC:38 cm ŌĆó Anterior fontanel: bulging and tense ŌĆó Weight: 2.5 KG ŌĆó Sub vitals ŌĆó A+ J- C- D+ E-
- 11. SYSTEMIC EXAMINATION: CNS: ’éó Poor primitive reflexes ’éó Poor Moro, poor sucking, rooting, grasping ’éó Tone was increased
- 12. CHEST EXAMINATION: On inspection: normal chest movements with respiration On palpation: no tenderness, mass, crepitus On percussion: resonant note On auscultation: B/L clear, N/V/B
- 13. ABDOMINAL EXAMINATION: On inspection: normal symmetry normal movement with respiration On palpation: no tenderness, rebound tenderness ,mass , no viceromegaly On percussion: tympanic note On auscultation: bowel sounds were audible
- 14. CARDIOVASCULAR EXAMINATION: ’éó Normal 1st and 2nd heart sounds ’éó Apex beat palpable at 5th intercostal space ’éó No any added sounds
- 15. ON INVESTIGATIONS: CBC showed ’éó Hb: 9.6 mg/dl ’éó WBC: 11500 mg/dl ’éó Plt: 210,000 mg/dl
- 16. SERUM U/C/E SHOWED ’éó Urea: 52 mg/dl ’éó Creatinine: 0.3 mg/dl ’éó Sodium: 122.5 mg/dl ’éó Potassium:5.9 mg/dl ’éó Chloride: 85.1 mg/dl ’éó Calcium: 9.7 mg/dl
- 17. IMAGING: U/S showed ’éó Moderately dilated all four ventricles ’éó Intraventricular septation ’éó Edema of brain parenchyma
- 19. DIFFERENTIAL DIAGNOSIS: ’éó Hydrocephalus ’éó Meningitis ’éó Encephalitis ’éó Chronic haemolytic anemia(thalasemia) ’éó Rickets ’éó Osteogenesis imperfecta ’éó Epiphyseal dysplasia
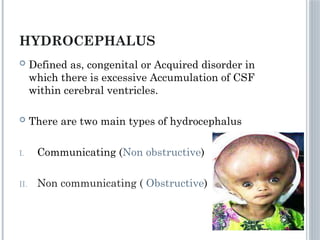
- 20. HYDROCEPHALUS ’éó Defined as, congenital or Acquired disorder in which there is excessive Accumulation of CSF within cerebral ventricles. ’éó There are two main types of hydrocephalus I. Communicating (Non obstructive) II. Non communicating ( Obstructive)
- 23. ETIOLOGY Congenital ’éó Congenital aqueductal stenosis ’éó Dandy walker malformation: Massive Dilation of fourth ventricle which obstructs Csf flow & there is hypoplasia of cerebellar vermis ’éó Arnold chiari malformation type II: The cerebellar tonsils are displaced downward and obstructs the Csf flow . ’éó Archnoid cyst or congenital tumours ’éó Intrauterine infections like CMV, Syphillis , toxoplasmosis
- 24. ACQUIRED HYDROCEPHALUS ’éó Secondary to infections of nervous systems e:g Bacterial meningitis ’éó ’éó Brain tumours ’éó Archnoiditis secondary to bleeding into subarchnoid space from a ateriovenous malformation , aneurysm or trauma. ’éó IntraventriculAr haemorrhage in preterm infants.
- 25. PHYSIOLOGY
- 26. CAUSES ’éó Increased production of CSF ’éó A block in CSF flow ’éó Impaired absorption of CSF ’éó ’éó Most common mechanism for producing hydrocephalus is impaired absorption of Csf due to obstruction of flow or dysfunction of absorptive mechanisms.
- 27. SIGNS & SYMPTOMS ’éó There are signs & symptoms of primary process I,e Infection , trauma,bleeding ’éó May be sign & symptoms of raised intracranial pressure secondary to normal pressure hydrocephalus. ’āś NonSpecific symptoms ’āś Headache, vomiting personality & behaviour changes ( irritable lethargy drowsiness) ’āś Nonspecific signs ’āś 3rd and 6th cranial nerve defecit, paresis of extraocular muscles leading to diplopia , there may be papilledema.
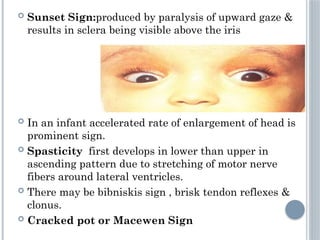
- 28. ’éó Sunset Sign:produced by paralysis of upward gaze & results in sclera being visible above the iris ’éó In an infant accelerated rate of enlargement of head is prominent sign. ’éó Spasticity first develops in lower than upper in ascending pattern due to stretching of motor nerve fibers around lateral ventricles. ’éó There may be bibniskis sign , brisk tendon reflexes & clonus. ’éó Cracked pot or Macewen Sign
- 29. INVESTIGATIONS ’éó X-ray ’éó CT scan ’éó MRI
- 30. ON CT
- 32. TREATMENT ’éó Includes specific therapy for any undertling disease ie(meningitis ,brain abcess, tumour) ’éó Medical therapy to decrease Csf production in slowly progresssive hydrocephalus includes Acetazolamide,foursemide & glycerol.
- 33. ’éó A ventriculo peitoneal shunt is created between ventricles and peritoneal cavity is the most effective surgical method of treating hydrocephalus ’éó Complications of shunt are mechanical obstruction of shunt are mechanical obstruction of shunt are meningitis or ventriculitis . Common organism is staph Epidermidis