Case Study - Medical Error.pptx
ŌĆóDownload as PPTX, PDFŌĆó
0 likesŌĆó84 views

Two patients had their biopsy results mixed up when the SHO wrote the consultant's findings on the wrong request forms. One patient was told he had benign prostatic hyperplasia when he actually had cancer and did not receive treatment for a year. The other patient received unnecessary radiotherapy after being told he had cancer when his biopsy showed BPH instead. An investigation found the consultant had made the correct diagnoses but the error was in recording the results. The case highlights the need for improved organizational processes, accountability, and a culture of patient safety to prevent such harmful medical errors.










Case Study - Medical Error.pptx
- 1. ŌĆ£Biopsy results of two patients mixed upŌĆØ
- 2. Objectives 1. Describe the case study 2. Describe the theoretical model 2. Analysis of the case for root causes 4. Study how to prevent its recurrence suggesting recommendations
- 3. Case Study Mr: O : Consultant Urologist Dr: P : SHO Pathology Dr: R : Consultant Pathologist Mr A & Mr B : Patients undergoing Trans-Rectal US guided needle biopsy of prostate.
- 4. Case Study ct.. ’éŚ Two prostatic biopsy samples : taken (from Mr A & Mr B); ’éŚ Each sample: labelled with relevant patientŌĆÖs details; ’éŚ Labelled samples: sent to path lab with relevant request forms; ’éŚ In the lab: slides were prepared; and sent to SHO with their relevant request forms; ’éŚ Each slide : examined first by SHO & findings noted down; ’éŚ Both slides : taken to const. pathologist; to be reviewed together; ’éŚ Diagnosis made; 1. Prostate Cancer 2. Benign Prostatic Hyperplasia (BPH)
- 5. Case Study ct.. ’éŚ Consultants findings: written on back of each patientŌĆÖs request form by SHO; ’éŚ Findings from each request form: taken to a tape; each tape was attached to corresponding request form; sent to secretary to computerize; computer reports were double checked and matched with request forms; ’éŚ Reports sent to cont. Urologist; ’éŚ Mr: A: No cancer (BPH); No treatment ’éŚ Mr: B: Adenocarcinoma; Radiotherapy
- 6. Identification of the medical error: ’éŚ One year later: Mr: A : High S. PSA; ’éŚ Repeat needle biopsy : adenocarcinoma diagnosed
- 7. Investigation: Mr AŌĆÖs previous slide : rechecked; ’éŚ found correctly labelled; slide showed a cancer; (but reported as BPH); Mr BŌĆÖs slide : ’éŚ showed BPH; (but reported as cancer); Conclusion of Investigation: ’éŚ Consultant had correctly diagnosed; ’éŚ But, SHO had written on wrong patients request form; ’éŚ Other biopsy slides, SHO had reported : were also rechecked; no errors
- 8. Disclosure: ’éŚ Mr: O (urologist) met each patient and apologized; ’éŚ explained what happened. Consequences: Two patients harmed by single slip up; ’éŚ One yearŌĆÖs delay in treating Mr A could significantly affect the prognosis; ’éŚ Mr B was subjected to an unnecessary course of radiotherapy. All other checks : invalidated by a single mistake resulting in great consequences.
- 9. A- Biopsy B-Biopsy A- Biopsy B-Biopsy one sample: benign one sample adeno carcinoma A- PSA gradually increasing A-no treatment follow up PSA B- Underwent radiotherapy A- Benign report B-adenocarcinoma of prostate A- Adeno carcinoma Ex by Dr P Ex by dr P & R Enter into com One year later Dr O Repea t Bx
- 10. Swiss cheese model of Accident causation In this model , errors made by individuals result in disastrous consequences due to flawed system- ŌĆ£the holes in the cheeseŌĆØ
- 11. Analysis of this case ’éŚ Active Error : Action slip/Action failure : (correct diagnosis written on the wrong request form) ’éŚ Latent Errors : 1. Failures in organizational process: Eg: ’éŚ Similar types of samples sent to the lab at one time, from one place; ’éŚ Samples placed in one tray.
- 12. Analysis Ct.. 2. Back ground factors: (Work load, Communication, Supervision etc) Eg: ’éŚ Identity of slides & request forms - not double checked by two personnel; ’éŚ No accountability of consultant for the accuracy of diagnosis; ’éŚ No computer reports checked against patient identification details and diagnosis on the request form
- 13. Recommendations Organizational process should be improved: ’éŚ Process mapping and documented clear guidelines to each level of the staff. ’éŚ Similar types of samples should be separated in the lab; ’éŚ They should be placed in separate trays; Back ground factors should be improved: ’éŚ ║▌║▌▀Ż matched with the identity on the request form by the consultant; ’éŚ Request forms signed by consultant for the accuracy of diagnosis ’éŚ Computer reports to be checked against both patient identification details and diagnosis on the request form.
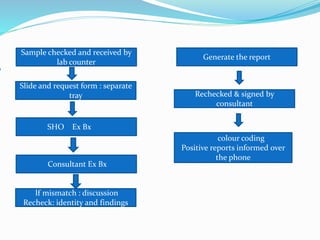
- 14. Sample checked and received by lab counter ║▌║▌▀Ż and request form : separate tray SHO Ex Bx Rechecked & signed by consultant Generate the report Consultant Ex Bx colour coding Positive reports informed over the phone lf mismatch : discussion Recheck: identity and findings
- 15. Recommendations ct.. ’éŚ Implement an Adverse Event Reporting System, system of root cause analysis with a constructive feed back system. ’éŚ Motivate staff to foster a Patient Safety Culture. ’éŚ Establish a culture where patient safety issues are discussed openly, staff and patients treated fairly; promoting learning & communicating experience to mitigate future incidents.
- 16. Summary ’éŚ Case Study of a Medical Error with mixed up lab reports. ’éŚ Two patients were harmed by single failure. ’éŚ Both Active Errors (Action failure) and Latent Errors (Failures in organizational process & Back ground factors) were identified as causative factors. ’éŚ Strengthening of Patient Safety Culture was recommended.
- 17. Thank You