Cementum
âĒDownload as PPT, PDFâĒ
1 likeâĒ318 views

Cementum is the calcified tissue covering the root of a tooth. It is avascular and composed of non-collagenous proteins and collagen fibers. There are different types of cementum including acellular and cellular cementum. Acellular cementum lacks cells and contains Sharpey's fibers, while cellular cementum contains cementoblast cells. Cementum is deposited throughout life to compensate for tooth eruption and wear. It attaches to the tooth and permits nutrient diffusion. Conditions like hypercementosis and cementum resorption can affect the amount and structure of cementum.









































Cementum
- 1. CEMENTUM
- 2. Cementum is calcified avascular mesenchymal tissue that forms the outer covering of the anatomic root.
- 3. COMPOSITION
- 4. NON COLLAGENOUS PROTEIN Bone sialoprotein,osteopontin,osteonectin-regulate mineralization and extend of crystal growth PDGF,IGF-promote cementum formation by altering cell cycle Fgf-cell proliferation and migration Cementum attachment protein-attachment of mesenchymalcells t o matrix
- 5. SOURCES OF COLLAGEN FIBRES Extrinsic fibres(Sharpeyâs fibres)-fibroblast Intrinsic fibres-cementoblast
- 8. TYPES OF CEMENTUM âĒ ACELLULAR âĒ CELLULAR
- 14. SHROEDERâS CLASSIFICATION OF CEMENTUM âĒ Acellular afibrillar cementum âĒ Acellular extrinsic fibre cementum âĒ Cellular mixed stratified cementum âĒ Cellular intrinsic fibre cementum âĒ Intermediate cementum
- 15. ACELLULAR AFIBRILLAR CEMENTUM During tooth eruption if there is loss of cervical part of reduced enamel epithelium mature enamel cap come in contact with surrounding connective tissue will deposit a layer of acellular afibrillar cementum. Contains neither cells nor extrinsic or intrinsic collagen fibres except for mineralized ground substance. Coronal cementum 1-15 micrometer thickness
- 16. ACELLULAR EXTRINSIC FIBRE CEMENTUM Lacks cells Bundles of sharpeyâs fibres present Found in the cervical third of root and extend apically Thickness- 30 â 230 micrometre Products of fibroblast and cementoblast
- 17. CELLULAR MIXED STRATIFIED CEMENTUM Composed of extrinsic and intrinsic fibres. May contain cells Appears in the apical third of the root and apices in the furcation areas Thickness- 100- 1000 micrometre.
- 18. CELLULAR INTRINSIC FIBRE CEMENTUM Contains cells Fills resorption lacunae No extrinsic collagen fibres
- 19. INTERMEDIATE CEMENTUM Poorly defined zone near cementodentinal junction of certain teeth that contain cellular remnants of hertwigs sheath embedded in calcific ground substance.
- 20. PERMEABILITY Acellular and cellular cementum are very permeable and permit the diffusion of dyes from the pulp and external root surface. In cellular cementum the canaliculi in some areas are contiguos with dentinal tubuli. Permeability diminishes with age.
- 21. CEMENTOENAMEL JUNCTION 60%-65% of cases , cementum overlaps the enamel. 30%edge to edge butt joint exits 5%-10% cementum and enamel fail to meet.
- 22. CEMENTODENTINAL JUNCTION âĒ The terminal apical area of cementum where it joins the internal root canal âĒ No increase or decrease in width with age âĒ Normal width 2-3 micrometre
- 23. THICKNESS OF CEMENTUM ï Cementum deposition is a continuos process. ï Proceed at varying rates throughout life. ï Most rapid formation at apical region to compensate eruption. ï Thickness on the coronal half 16-60 micrometres ï Apical one third and furcation- 150-200 micrometres. ï Thicker on the distal surface than on the mesial (tooth tendency to mesial drift) ï From 11 to 70 years average thickness increases 3 times ï Average thickness 95micrometer at age of 20yrs and 215micrometer at age of 60yrs
- 24. HYPERCEMENTOSIS ï Abnormal prominent thickening of the cementum with nodular enlargement of apical third. ï It can be diffuse or circumscribed. ï Affect all teeth or may be confined to single tooth. ï Age related phenomenon.
- 25. ETIOLOGY OF HYPERCEMENTOSIS âĒ Local ïž Excessive tension from orthodontic appliances ïž Excessive tension from occlusal forces ïž Teeth without antagonist ïž Periapical irritation ïž Benign cementoblastoma ïž Cementifying fibroma ïž Periapical cemental dysplasia ïž Fibro cementoosseous dysplasia
- 26. âĒ Systemic ïž Pagets disease ïž Acromegaly ïž Calcinosis ïž Rheumatic fever ïž Thyroid goiter o Also oours as ageneralized thickening of cementum without nodular enlargement ofapical third of root o Also appear as cemental spikes
- 27. If overgrowth improves the functional qualities of the cementum it is called cementum hypertrophy. If overgrowth occurs in nonfunctional teeth or if it is not correlated with increased function it is termed as hyperplasia. It can also be seen as knob like projections- excementoses
- 28. RADIOGRAPHIC FEATURES Radiographically radiolucent shadow Of PDL and radiopaque lamina dura are seen in the outter border of area of hypercementosis In cases of periapical cemental dysplasia ,condensing osteitis and focal periaplical osteoporosis it can be differentiaited radiographically as al these entities are located outside the shadow of PDL and lamina dura
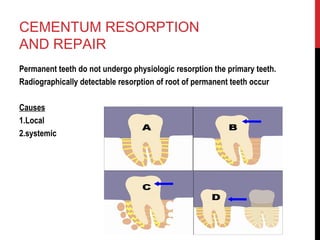
- 29. CEMENTUM RESORPTION AND REPAIR Permanent teeth do not undergo physiologic resorption the primary teeth. Radiographically detectable resorption of root of permanent teeth occur Causes 1.Local 2.systemic
- 30. CAUSES local ï trauma from occlusion ï Orthodontic movement ï Pressure from malaligned teeth ï Cysts and tumors ï Teeth without functional antagonist. ï Embedded teeth ï Reimplanted /transplanted teeth. ï Periapical disease ï Periodontal disease
- 31. Systemic ïCalcium deficiency ïHypothyroidism ïPagetâs disease ïHereditary fibrous osteodystrophy
- 32. CEMENTUM RESORPTION They appear microscopically like bay like concavities in root surface. Multinucleated giant cells and large mononuclear macrophage are seen nearby. Several small areas of destruction coalesce to form large areas of destruction. Resorption may extend to dentin and even pulp
- 33. Usually painless May alter with periods of repair which produce reversal line Cementum repair can occur in vital and non vital teeth (cementum repair from external blood supply and not from pulp) External blood supply includes from alveolar bone and periodontal ligament and blood vessel.
- 34. REVERSAL LINE âĒ Newly formed cementum is demarcated from the root by deeply staining irregular lines called reversal lines. âĒ It contains few collagen fibrils and ore proteoglycans and mucopolysacchrides âĒ Embeded fibres of periodontal ligament reestablish functional relationship with new cementum.
- 35. ANKYLOSIS It is an abnormal repair Fusion of cementum and alveolar bone with obliteration of periodontal ligament. Cause - ï Chronic periapical infection ï Tooth reimplantation ï Occlusal trauma ï Around embedded tooth ï submerged
- 36. âĒClinically- lack physiologic mobility Metallic sound Teeth in infraocclusion No physiologic drifting âĒXray- Missing pdl space
- 37. EXPOSURE OF CEMENTUM TO ORAL CAVITY Occurs due to recession Cementum permeable to be penetrated by organic substance inorganic ions Bacteria Caries can also develop.
- 38. FUNCTIONS âĒ Attachment medium â binds tooth to the bone though sharpeyâs fibres. âĒ Continous deposition âĒ Repairative tissue- it acts as a repairative organ. âĒ Functional adaptation- occlusal wear compensation âĒ Protect the dentin âĒ Help in eruption process
- 39. CONCLUSION âĒ Cementum is calcified avascular mesenchymal tissue that covers anatomic portion of root. It provide anchorage to principal fibers of PDL.It also plays a role in maintaining occlusal relationship.Cementum when lose the protective coveing of alveolar bone and gingiva, it get exposed to oral environment ,bacterial penetration and thereby caries.
- 40. BIBLIOGRAPHY âĒ CLINICAL PERIODONTOLOGY-CARRANZA âĒ ORAL HISTOLOGY-TENCATE âĒ ORAL BIOLOGY âMAJI JOSE
- 42. MCQâS 1. Acellular cementum seen in a) Coronal portion of root b) Apical portion of root c) Middle portion of root d) At CEJ 2. Collagen fibres are absent in a) AEFC b) AAC c) AMSC d) Intermediate cementum
- 43. 3 . Edge to edge contact of cementum and enamel occur in a) 10% b) 30% c) 50% d) 5% 4. Sharpeyâs fibres are derived from a) Fibroblast b) Cementoblast c) Mesenchymal cells d) osteoblast
- 44. 5. Feature of ankylosed teeth a) Lack of physiologic mobility b) Teeth in infra occlusion c) Metallic sound d) All the above