




























































cholera and diarrhoea
- 1. WELCOME
- 2. GUIDED BY JHANSI RUTH MADAM PRINCIPAL OF ANRI COLLEGE OF NURSING PRESENTED BY MS.B.HEMALATHA B.SC NURSING 4TH YEAR
- 5. INRODUCTION Every year more than 10 million children die in developing countries before they reach their fifth birthday. 7 in 10 of these deaths are due to acute respiratory infections (mostly pneumonia) , diarrhoea, measles, malaria, or malnutrition and often to a combination of these illness.
- 6. DEFINITION
- 7. DEFINITION Diarrhoea is defined as the passage of loose ,liquid or watery stools .These liquid stools are usually passed more than three times a day . However , it is the recent change in consistency and character of stools rather than the number of stools that is more important.
- 8. TYPES
- 10. 1. ACUTE WATERY DIARRHOEA: It lasts several hours to days , the main danger is dehydration , weight loss also occurs if feeding is not continued. The pathogens that cause acute diarrhoea that include v.cholera or E.coli
- 11. 2.ACUTE BLOODY DIARRHOEA: It is also called as dysentry , this damages the intestinal mucosa , sepsis and malnutrition other coomplications including dehydration may also occur. Marked as visible blood in stools common cause of bloody diarrhoea is shigella.
- 12. 3.PERSISTENT DIARRHOEA: This lasts for 14 days or longer the main danger is serious malnutrition and serious non intestinal infection , dehydration may also occur.
- 13. 4.DIARRHOEA WITH SEVERE MALNUTRITION: The main dangers are severe infection , dehydration , heart failure, vitamin and mineral deficiency.
- 15. EPIDEMIOLOGY ÔÉò Acute diarrhoea is revealed in importance only by respiratory infection , as a cause of morbidity on a world wide scale. ÔÉò When the WHO initiated the diarrhoeal diseases control programme in 1980 , approximately 4.6 million children used to die in each year of the dehydration caused by diarrhoea. ÔÉò During the year 2011 about 10.6 million cases with 1223 deaths were reported in India.
- 16. AGENT FACTORS % OF CASES • Virus • Bacteria • Rotavirus • E.coli • Shigella • Campylobacter • Vibrio cholera • salmonella 15 -25 10-20 5-15 10-15 5-10 1-5 PATHOGEN
- 20. Agent factors % OF CASES • Virus • Bacteria • Rotavirus • E.coli • Shigella • Campylobacter • Vibrio cholera • salmonella 15 -25 10-20 5-15 10-15 5-10 1-5 PATHOGEN
- 21. RESERVOIR OF INFECTION ÔÉòMan is the reservoir for some enteric pathogens and thus most transmission occurs from human factors.eg: E.coli, shigella. ÔÉòAnimals are important reservoir and transmission originates from both human and animal faeces. e.g.: campylobacter, salmonella.
- 23. HOST FACTORS Diarrhoea is the most common in children especially in those between 6months and 2 years. Incidence is highest in the age group 6-11 months, when weaning occurs. It is also common in babies under 6 months of age fed on cow’s milk.
- 24. ENVIRONMENTAL FACTORS In temperature climate, bacterial diarrhoea occur more frequently during the warm season where as viral diarrhoea caused by rotavirus peak during the winter.
- 26. MODE OF TRANSMISSION Diarrhoea in many countries are transmitted primarily or exclusively by the faeco-oral route. Its transmission may be water borne, food borne or direct transmission.
- 29. CONTROL OF DIARRHOEAL DISEASE The diarrhoeal diseases control programme of WHO has since its inception in 1980. Components of a diarrhoeal disease control programme: 1. Short term: a. Appropriate clinical management 2. Long term: a. Better MCH care practices b. Preventive strategies c. Preventing diarrhoeal diseases
- 30. APPROPRIATE CLINICAL MANAGEMENT Oral rehydration therapy: The aim of oral fluid therapy is to prevent dehydration and reduce mortality. It has been proved that 90to 95 percent of all cases of cholera and acute diarrhoea can be treated by oral fluids alone.
- 31. Oral Rehydration therapy To prevent dehydration and reduce mortality. REDUCED OSMOLALITY ORS gms/liter ÔÇß Sodium chloride ÔÇß Glucose, anhydrous ÔÇß Potassium chloride ÔÇß Trisodium citrate, dehydrate TOTAL WEIGHT IS ÔÇß 2.6 ÔÇß 13.5 ÔÇß 1.5 2.9 20.5
- 32. REDUCED OMOLARITY ORS+ m mol/litre Sodium Chloride Glucose, anhydrous Potassium Citrate total is 75 65 75 20 10 245
- 33. A simple mixture consisting of Table salt 5gm Sugar 20gm dissolved in 1 litre of boiled drinking of water which is safely used until the mixture is obtained. PREPARATION OF ORS
- 35. INTRAVENOUS REHYDRATION The solutions recommended by WHO for intravenous infusions are : Ringer’s lactate solution(Hartman's solution) It can correct dehydration due to acute diarrhoea of all cases.
- 36. a. BETTER MCH CARE PRACTCES ÔÉòMaternal nutrition ÔÉòChild nutrition o Promotion of breast feeding o Appropriate weaning practices o Supplementary feeding o Vitamin A supplementation.
- 37. b. PREVENTIVE STRATEGIES • Immunization: Immunization against measles is a potential intervention for diarrhoeal control. when administered at the recommended age, the measles vaccine can prevent up to 25 percent of diarrhoeal deaths in children under 5 years of age. Rotavirus vaccine.
- 39. DIARRHOEAL DISEASE CONTROL PROGRAMME IN INDIA It was started in the year 1978 with the objective of reducing the mortality and morbidity due to diarrhoeal diseases. Since 1985- 1986 , with the inception of the national oral rehydration therapy programme.
- 41. INTRODUCTION cholera is an acute diarrhoeal disease caused by v.cholera 01 and 0139 . Typical cases are characterised by the sudden onset of profuse , effortless , watery diarrhoea followed by vomiting , rapid dehydration , muscular cramps and suppression of urine. unless there is rapid replacement of fluid and electrolytes , the case fatality may be as high as 30 to 40 percent.
- 43. DEFINITION An infectious sometimes fatal disease of the small intestine caused by the bacterium vibrio.cholera. It is spread from contaminated water and food and causes severe diarrhoea , vomiting and dehydration.
- 44. INCIDENCE The number of cholera cases reported to WHO continues to risk for 2011 alone , a total cases of 589,854 cases were notified. Cholera remains a global threat to public health and a key indicator of lack of social development.
- 46. EPIDEMIOLOGICAL FEATURES Cholera is both an epidemic and endemic disease. AGENT-vibrio cholera HOST- ENVIRONMENTAL All ages and both gender FACTORS-poor
- 47. MODE OF TRANSMISSION Transmission occurs from man to man via  Faecally contaminated  Contaminated food and drinks  Direct contact.
- 49. INCUBATION PERIOD From a few hours up to 5days , but commonly 1-2 days.
- 51. CLINICAL FEATURES The severity of cholera is dependant on the rapidly and the duration of fluid loss. it shows three stages: 1.stage of evacuation: the onset is abrupt with profuse , painless, watery diarrhoea followed by vomitting.The patient may pass as many as 40 stools in a day.
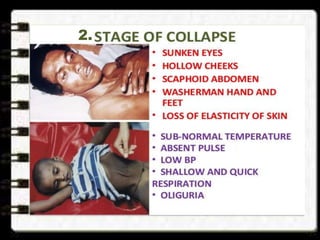
- 52. 2.Stage of collapse: The patient soon passes into a stage of collapse because of dehydration. signs are:  sunken eyes  hollow cheeks Scaphoid abdomen Sub normal temperature Washerman’s hand and feet Absent pulse 2.
- 53. 3.Stage of recovery: if death does not occur the patient shows signs of clinical improvement. B.p begins to raise, temperature returns to normal ,and urine secretion is re- established. if anuria persists the patient may die of renal failure. severe cholera occurs in 5 to 10 percent of cases.
- 54. LABORATORY DIAGNOSIS ÔÉò Collection of stool ÔÉòCollection of vomitus ÔÉòWater ÔÉò food samples ÔÉòTransportation ÔÉòDirect examination ÔÉòCulture method
- 55. CONTROL OF CHOLERA 1.verification of the diagnosis: confirmation of the diagnosis as early as possible. 2.Notification: Educate the vulnerable group regarding the disease. 3.Early case finding: an aggressive search for the cases should be made in the community.
- 56. 4.Establishment of treatment centers: The mild dehydrated patients should be treated at home with ORS .Severely dehydrated patients requiring intravenous fluids. 5.Rehydration therapy: mortality rate have been brought down to less than by effective rehydration therapy.
- 57. 6.Adjuncts to therapy: antibiotics should be given as soon as vomitting has stopped which is usually after 3 to 4 hours of oral rehydration.ex- fluoroquinolones , tetracycline , ampicilline. 7.sanitation measures: o Water control o Excreta disposal o Food sanitation o disinfection
- 59. HEALTH EDUCATION  The effectiveness and simplicity of oral rehydration therapy. Isolation and early notification. Food hygiene practices. Hand washing after defecation and before eating.
- 60. DIARRHOEAL DISEASE CONTROL PROGRAMME The incidence of cholera cases and deaths has decreased in recent years. During the year 1980- 1981 strategy of national cholera control programme termed as diarrhoeal disease control programme. main aim: To prevent death due to dehydration.
- 63. THANK YOU ALL