


![ŌĆó A cough is an innate primitive reflex and acts as part of the bodyŌĆÖs
immune system to protect against foreign materials.
ŌĆó It starts as a deep inspiration, followed by a strong expiration
against a closed glottis, which then opens with an expulsive flow of
air, followed by a restorative inspiration
Sharma S, Hashmi MF, Alhajjaj MS. Cough. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls
Publishing; 2023 Jan-.](https://image.slidesharecdn.com/chrcoughfinal-240531060955-553b3e2b/85/Chronic-Cough-Presentation-by-DR-Aiswarya-Thambi-Pulmonologist-pptx-4-320.jpg)















![COUGH CHARACTERISTICS ACCORDING TO
ETIOLOGY
ŌĆó UACS [POST NASAL DRIP SX] sensation of throat clearing
ŌĆōpharyngitis/sinusitis
ŌĆó GERD ŌĆō reflux ŌĆōcan be cause of cough -1 of 3 common
cause of chronic cough -25% cases ŌĆōmay or maynot a/w
typical symptoms ŌĆōheartburn or regurgitation](https://image.slidesharecdn.com/chrcoughfinal-240531060955-553b3e2b/85/Chronic-Cough-Presentation-by-DR-Aiswarya-Thambi-Pulmonologist-pptx-22-320.jpg)
































![COMPLICATION OF COUGH
ŌĆó Chest pain [myalgia]
ŌĆó Fractures of ribs [COPD]
ŌĆó Urinary incontinence
ŌĆó Hernia
ŌĆó Sub conjunctival hemorrhage
ŌĆó Cough syncope](https://image.slidesharecdn.com/chrcoughfinal-240531060955-553b3e2b/85/Chronic-Cough-Presentation-by-DR-Aiswarya-Thambi-Pulmonologist-pptx-55-320.jpg)


Chronic Cough Presentation by DR Aiswarya Thambi Pulmonologist.pptx
- 1. CHRONIC COUGH DR AISWARYA THAMBI MBBS MD DNB PULMONOLOGY CONSULTANT PULMONOLOGIST DAYA HOSPITAL,TCR
- 2. OVERVIEW ŌĆó Epidemiology ŌĆó Etiology ŌĆó Red flag signs ŌĆó Evaluation ŌĆó Management ŌĆó Conclusion
- 4. ŌĆó A cough is an innate primitive reflex and acts as part of the bodyŌĆÖs immune system to protect against foreign materials. ŌĆó It starts as a deep inspiration, followed by a strong expiration against a closed glottis, which then opens with an expulsive flow of air, followed by a restorative inspiration Sharma S, Hashmi MF, Alhajjaj MS. Cough. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
- 5. PHASES OF COUGH (1) A DEEP INITIAL INSPIRATION, (2) COMPRESSION OF AIR IN THE LUNGS AND AIRWAYS BY FORCEFUL CONTRACTION OF THE EXPIRATORY MUSCLES COUPLED WITH TIGHT CLOSURE OF THE GLOTTIS AND OPENING OF THE LARYNX, AND (3) SUDDEN EXPLOSIVE EXPIRATION FOLLOWED BY NARROWING OF THE GLOTTIS AND RETURN OF THE LARYNX TO ITS NORMAL INSPIRATORY POSITION. 5
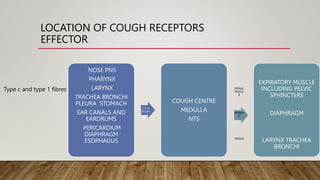
- 6. LOCATION OF COUGH RECEPTORS EFFECTOR NOSE PNS PHARYNX LARYNX TRACHEA BRONCHI PLEURA STOMACH EAR CANALS AND EARDRUMS PERICARDIUM DIAPHRAGM ESOPHAGUS 5 9 10 phrenic COUGH CENTRE MEDULLA NTS SPINAL MOTO R PHREN IC VAGUS EXPIRATORY MUSCLE INCLUDING PELVIC SPHINCTERS DIAPHRAGM LARYNX TRACHEA BRONCHI Type c and type 1 fibres
- 8. ŌĆó The community prevalence of chronic cough is unclear, perhaps as high as 10%. ŌĆó Many sufferers donŌĆÖt access medical services, tolerating symptoms or possibly self-medicating. ŌĆó UK based primary care studies suggest chronic cough affecting 1.2-2% of the population but it is most likely under-estimated. BTS Clinical statement on chronic cough in adults- 2022
- 9. IMPACT OF CHRONIC COUGH Anxiety Work- absenteeis m Impact on quality of life Multiple health care visits BTS Clinical statement on chronic cough in adults- 2022
- 10. TYPES OF COUGH
- 11. Acute < 3 weeks Sub ŌĆō Acute 3- 8 weeks Chronic > 8 weeks Irwin RS , Baumann MH , Bolser DC , et al . Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest 2006;129:23S.doi:10.1378/chest.129.1_suppl.1S
- 12. WHAT IS NEW?
- 13. Refractory chronic cough ŌĆó Cause - identified ŌĆó Persists despite treatment of treatable traits ŌĆó May have symptoms of cough hypersensitivity Refractory unexplained chronic cough ŌĆó Cause- unknown ŌĆó No treatable traits ŌĆó No symptoms suggestive of cough hypersensitivity Cough hypersensitivity syndrome ŌĆó Triggered by low levels of thermal, mechanical, or chemical exposure. ŌĆó mediated by sensitisation of the sensory neuronal pathways controlling cough including the vagus nerve and central nervous system BTS Clinical statement on chronic cough in adults- 2022
- 14. When you cough repeatedly it can result in 'overstimulation' of the nerve, causing the nerve to become hypersensitive, which means it triggers more frequently than normal. A number of factors, including viruses and certain medications, can also have a direct impact on the cough reflex nerve, making it more sensitive. COUGH HYPERSENSITIVITY
- 16. ACUTE COUGH SUB-ACUTE COUGH CHRONIC COUGH 1) acute viral upper respiratory infection, 2) acute bronchitis, 3) acute rhinosinusitis, 4) pertussis, 5) acute exacerbations of chronic obstructive pulmonary disorder, 6) allergic rhinitis, 7) asthma, 8) congestive heart failure, 9) pneumonia, aspiration syndromes, and 10)pulmonary embolism 1) most commonly post-infectious secondary to continued irritation of cough receptors via ongoing or resolving bronchial or sinus inflammation from a preceding viral upper respiratory infection. 1) upper airway cough syndrome, 2) gastroesophageal reflux disease, 3) non-asthmatic eosinophilic bronchitis, 4) chronic bronchitis, 5) postinfectious cough, 6) intolerance to angiotensin- converting enzyme inhibitor medication, 7) malignancy, 8) interstitial lung diseases, 9) chronic sinusitis, and 10)psychosomatic cough.
- 17. ŌĆó Acute cough may suggest: ŌĆó Upper RT ŌĆó Common cold ŌĆó Sinusitis ŌĆó Lower RT ŌĆó Pneumonia ŌĆó Bronchitis ŌĆó Exacerbation of COPD /asthma ŌĆó Inhalation of bronchial irritant (eg, smoke or fumes ŌĆó CHF ŌĆó PULMONARY EMBOLISM ŌĆó SUDDEN ONSET VIOLENT COUGH ESP IN CHILDŌĆō INHALATION OF FOREIGN BODY ACUTE COUGH
- 19. SUBACUTE COUGH 3-8 WEEKS ŌĆó Postinfectious MC ’üČA cough that begins with an acute respiratory tract infection and is not complicated* by pneumonia ’üČ *Not complicated = Normal lung exam normal chest X-ray ’üČGenerally cough is non productive ’üČResolve without treatment SINUSITIS Asthma
- 21. CHRONIC COUGH 1) Upper Airway Cough Syndrome, 2) Gastroesophageal Reflux Disease, 3) Non-asthmatic Eosinophilic Bronchitis, 4) Chronic Bronchitis, 5) Postinfectious Cough, 6) Intolerance To Angiotensin-converting Enzyme Inhibitor Medication, 7) Malignancy, 8) Interstitial Lung Diseases, 9) Chronic Sinusitis, And 10)Psychosomatic Cough.
- 22. COUGH CHARACTERISTICS ACCORDING TO ETIOLOGY ŌĆó UACS [POST NASAL DRIP SX] sensation of throat clearing ŌĆōpharyngitis/sinusitis ŌĆó GERD ŌĆō reflux ŌĆōcan be cause of cough -1 of 3 common cause of chronic cough -25% cases ŌĆōmay or maynot a/w typical symptoms ŌĆōheartburn or regurgitation
- 23. ASTHMA ŌĆō sometimes cough me be its only symptom / atopic history /allergic skin tEsts should be documented DIAGNOSIS ŌĆōconfirmed by demonstration of variable airway obstruction FEV1>=12% and >=200ml improvement 15 min after use of bd and >20% after 10 to 14 days of treatment with corticosteroids PEF >=20% improvement postbronchodilator METHACHOLINE CHALLENGE TEST ŌĆō 20% DROP IN FEV1
- 24. ŌĆó CHRONIC BRONCHITIS ŌĆōCOUGH WITH SPUTUM EXPECTORATION FOR ATLEAST 3 CONSECUTIVE MONTHS FOR ATLEAST 2 CONSECUTIVE YEARS ŌĆó NON ASTHMATIC EOSINOPHILIC BRONCHITIS ŌĆōpatient present with bronchial eosinophilia on sputum analysis without bronchial hyperresponsiveness . Cough responds to ICS , just as does in asthma ŌĆó Cough caused by medication ŌĆōnon productive resolves within 4 weeks of stopping medication .affects 5-20% pt receiving ACE . BETA BLOCKERS ŌĆōc/c cough ŌĆō often by aggravating underlying asthma ŌĆó POSTINFECTIOUS COUGH ŌĆō Respiratory infection is often the cause of a/c or suba/c cough , accounts for about 15% of c/c cough cases
- 25. COUGH WITH POSTURAL VARIATION ŌĆó Sinusitis ŌĆó GERD ŌĆó Bronchectasis ŌĆó Lung abscess ŌĆó Pulmonay edema due to heart failure
- 26. COUGH WITH DIURNAL VARIATION ŌĆó Early morning cough ŌĆō ASTHMA , BRONCHIECTASIS ,C/C BRONCHITIS ŌĆó Nocturnal cough -- GERD , PULMONAY EDEMA ,TROPICAL PULMONARY EOSINOPHILIA
- 27. MECHANISM OF DRUG INDUCED COUGH ACEI -- Accumulation of bradykinin BETA BLOCKERS ŌĆō Causing bronchospasm BLEOMYCIN , BUSULFAN , AMIODARONE ŌĆō Lung fibrosis
- 28. ŌĆó All presumptive tb patients evaluated for sputum smear examination ŌĆó presumptive tb ŌĆó Cough>2weeks ŌĆó Fever>2weeks ŌĆó Significant weight loss ŌĆó hemoptysis TB
- 30. Red flag signs!
- 31. WATCH OUT! ŌĆó Impaired general condition, ŌĆó Recurrent infectious syndrome, ŌĆó Exertional dyspnea, ŌĆó Hemoptysis ŌĆó Cough appearance or change in cough in a smoker, ŌĆó Dysphonia, ŌĆó dysphagia, ŌĆó Cervical adenopathy, ŌĆó Abnormal cardiopulmonary / ENT examination ŌĆó Abnormal chest x-ray. L.Guilleminault,S.Demoulin-Alexikova,L.deGaboryetal. RespiratoryMedicineandResearch83(2023)101011
- 32. HEMOPTYSIS ŌĆó COUGHING up OF BLOOD ŌĆó Bright red ŌĆó Mixed with frothy sputum ŌĆó Alkaline ph ŌĆó Contains alveolar macrophages laden with hemosiderin
- 34. ŌĆó Cough: onset, duration, character, triggers ŌĆó Sputum-volume & character ŌĆó Postural variation ŌĆó Smoking, occupation ŌĆó Drug history
- 36. L.Guilleminault,S.Demoulin-Alexikova,L.deGaboryetal. RespiratoryMedicineandResearch83(2023)101011
- 37. L.Guilleminault,S.Demoulin-Alexikova,L.deGaboryetal. RespiratoryMedicineandResearch83(2023)101011
- 38. CAN YOU MEASURE COUGH?
- 39. Measurement of cough Cough reflex Cough frequency & intensity Quality of life questionnaire Subjective ŌĆō visual analogue scale French CT, Irwin RS, Fletcher KE, Adams TM: Evaluation of a cough specific quality-of-life questionnaire. Chest 121:1123ŌĆō1131, 2002
- 40. The Leicester Cough Questionnaire uses a seven- point Likert response scale for 19 items from three domains physical, psychological, and social And is shown to be repeatable and sensitive in patients with chronic cough Birring SS, Matos S, Patel RB, et al: Cough frequency, cough sensitivity and health status in patients with chronic cough. Respir Med 100:1105ŌĆō1109, 2006
- 41. MANAGEMENT
- 42. CLINICAL PRACTICE POINTS ŌĆó Establish who needs specialist referral or can be initially managed in general practice with a targeted trial of therapy. ŌĆó ŌĆśRed flagsŌĆÖ should prompt urgent referral ŌĆó The history should identify possible underlying disease and treatable traits. ŌĆó All patients with chronic cough should have a chest x ray (CXR), full blood count (FBC), diagnostic spirometry and exhaled nitric oxide (FeNO) (if available) BTS Clinical statement on chronic cough in adults- 2022
- 43. ACUTE COUGH
- 44. Self care Honey Herbal medicines Over the counter antitussives Over the counter expectorants NSAIDS Antihistamines decongestants NICE guidelines 2019 ŌĆō Acute cough
- 45. WHAT DOES THE EVIDENCE SAY?
- 46. MEDICATION EVIDENCE 1) Over the counter expectorants there was some evidence that suggests guaifenesin reduced cough symptoms in adults and young people with an acute cough or upper respiratory tract infection, with no increase in adverse effects 2) Over the counter antitussives a) the evidence for dextromethorphan was mixed. b) codeine had no benefit on cough symptoms. 3) Anti histamines and decongestants antihistamines and decongestants had no benefit on cough symptoms, and increased adverse effects 4) Bronchodilators bronchodilators, such as oral or inhaled salbutamol, did not benefit cough symptoms and increased adverse events, such as tremor
- 48. TREATABLE TRAITS OF CHRONIC COUGH
- 49. BTS Clinical statement on chronic cough in adults- 2022
- 50. S.NO Treatable trait Identification marker Treatment Outcome 1) Smoking Patient history. Urinary Cotinine. Exhaled CO. Smoking cessation. Nicotine replacement therapy (NRT). Resolving chronic bronchitis improvement in cough. May get worse initially as nicotine suppresses cough reflex. 2) Irritant exposure: cigarette smoking/vaping, occupational exposures chemical/particulates History Occupational history Reduce exposure May improve cough 3) ACEI Treatment History. Medication records Stop ACEI in all patients with chronic cough. Can use A2RB if needed instead Improvement in cough, may take 4 weeks or more. BTS Clinical statement on chronic cough in adults- 2022
- 51. SNO Treatable trait Identification Treatment outcome 4) Airway eosinophilia History FeNO > 25ppb Blood eosinophil counts > 0.3 * 109 / L) Inhaled or oral corticosteroids Improve cough and QoL Reduced exacerbations 5) Productive cough History of significant sputum production. Sputum C&S HRCT ? bronchiectasis Airway Clearance physiotherapy Mucolytics Antimicrobials Macrolides Limited evidence. May improve cough BTS Clinical statement on chronic cough in adults- 2022
- 52. SNO TREATABLE TRAIT IDENTIFICATION TREATMENT OUTCOME 6 Chronic rhinosinusitis History of two or more symptoms for Ōēź12 weeks, one of which should be either nasal blockage or nasal discharge (anterior or posterior), with or without facial pain/pressure or reduction or loss of smell Nasal steroids Saline douching Consider ENT referral Improvement in rhinosinusitis. Possible improvement in cough. Limited evidence. 7) Inducible laryngeal obstruction History Laryngoscopy Speech therapy May improve cugh BTS Clinical statement on chronic cough in adults- 2022
- 53. SNO Treatable traits Identification Treatment Outcome 8) Gastroesophageal reflux disease Clinical history presence of heartburn best indicator of possible response to treatment. Reflux Symptoms Oesophageal manometry Endoscopy PPIs Lifestyle measures Also consider; H2 antagonists, weight loss Fundoplication Limited evidence. May improve cough for a subgroup of patients. Most donŌĆÖt improve. 9) Obstructive sleep apnea History Sleep study CPAP therapy May improve cough Limited evidence BTS Clinical statement on chronic cough in adults- 2022
- 54. PSYCHOGENIC COUGH ŌĆó A diagnosis of exclusion ŌĆó Most common in adolescents with concomitant emotional disorders ŌĆó Does not produce sputum ŌĆó Usually does not occur at night ŌĆó Not affected by commonly used cough suppresants
- 55. COMPLICATION OF COUGH ŌĆó Chest pain [myalgia] ŌĆó Fractures of ribs [COPD] ŌĆó Urinary incontinence ŌĆó Hernia ŌĆó Sub conjunctival hemorrhage ŌĆó Cough syncope
- 56. SUMMARY ŌĆó A detailed history & clinical examination gives clues to the underlying disease ŌĆó Presence of red flag signs warrants thorough investigation. ŌĆó Judicious use of antibiotics is recommended ŌĆó Patients and family members are to be counselled accordingly.
- 57. THANK YOU!