Claviclefrctures
Download as ppt, pdf1 like307 views
This document discusses clavicular fractures. It begins with relevant anatomy of the clavicle and mechanisms of injury. It then describes classifications of fractures, with midshaft fractures being most common. Clinical history, imaging, and treatment options are outlined for different fracture types. Conservative treatment is generally recommended for medial fractures while immobilization or closed/open reduction may be used for midshaft fractures. Lateral fractures are also discussed along with complications. The conclusion emphasizes counseling for most fractures but certain types like displaced midshaft fractures may require operative intervention.
1 of 24
Downloaded 20 times


Ad
Recommended
Fracturas de Femur Distal
Fracturas de Femur DistalCarlos Brambila
╠²
El documento aborda las fracturas distales del f├®mur, describiendo su complejidad, mecanismos de lesi├│n y tratamientos actuales, los cuales incluyen t├®cnicas de osteos├¡ntesis para facilitar la recuperaci├│n. Se trata del manejo de estas fracturas, que representan el 7% de todas las fracturas de f├®mur, y se discuten las complicaciones tard├¡as como pseudoartrosis y rigidez. Tambi├®n se presentan preguntas para evaluar el conocimiento sobre la clasificaci├│n y tratamiento de estas lesiones.Distal radioulnar joint injuries
Distal radioulnar joint injuriesSunil Poonia
╠²
This document discusses distal radioulnar joint (DRUJ) injuries. It begins by providing background on the anatomy and biomechanics of the DRUJ. It then describes the clinical evaluation and various imaging modalities used to assess DRUJ injuries. The document presents classifications for triangular fibrocartilage complex injuries and DRUJ injuries associated with fractures. Treatment options are discussed, including non-operative treatment, arthroscopic and open surgical procedures. Specific injuries like isolated DRUJ dislocations, ulnar styloid fractures, Galeazzi fracture-dislocations, and chronic DRUJ instability are also reviewed.Degenerative Disc Disease
-
360 Spinal Fixation
Degenerative Disc Disease
-
360 Spinal FixationAlexander Bardis
╠²
The document provides an overview of degenerative disc disease, detailing its diagnosis, treatment options, and surgical interventions. It discusses conservative and operative treatments including various spinal fixation techniques and evaluations through clinical and imaging studies. Key factors for surgical intervention include unresponsive pain, neurologic deficits, and significant restrictions in daily activities.Hoffa Fracture(Bagaria Classification, Diagnosis and Management) PPT
Hoffa Fracture(Bagaria Classification, Diagnosis and Management) PPTHarshitSingha1
╠²
The document provides an overview of Hoffa's fracture, describing its definition, mechanism of injury, clinical examination, management strategies, and a new classification system known as the Bagaria classification. It emphasizes the importance of accurate diagnosis through imaging and the necessity of surgical intervention for effective treatment. Additionally, it outlines various surgical approaches and fixation methods tailored to the fracture's characteristics.Distal Radioulnar Joint (DRUJ) Injuries
Distal Radioulnar Joint (DRUJ) InjuriesKaushik Velugoori
╠²
This document discusses injuries to the distal radioulnar joint (DRUJ). It begins with an overview of the anatomy of the DRUJ and its importance. It then describes various types of DRUJ injuries including acute dislocations or injuries associated with fractures. Chronic injuries and arthritis are also discussed. Evaluation methods like imaging and clinical exams are provided. The classification and treatment options for different DRUJ injuries are explained, including non-operative and surgical treatments like repair, reconstruction or resection procedures.MANAGEMENT_OF_CLAVICLE_FRACTURE_AND_ACROMIOCLAVICULAR_INJURY 2.pptx
MANAGEMENT_OF_CLAVICLE_FRACTURE_AND_ACROMIOCLAVICULAR_INJURY 2.pptxmaneesh64
╠²
This document summarizes the presentation on clavicle fractures by Dr. K Maneesh Chandra. It discusses the mechanisms of injury, physical exam findings, imaging modalities, anatomy, treatment options and management of complications for clavicle fractures in infants, children and adults. Surgical treatment involves open reduction and internal fixation with plates or screws while non-surgical treatment uses sling immobilization. Complications are addressed and factors influencing treatment choice are outlined.Scaphoid fracture and nonunion
Scaphoid fracture and nonunion adityachakri
╠²
The document provides an overview of scaphoid fractures and their management, detailing anatomy, mechanisms of injury, diagnostic methods, and treatment options. It highlights the significance of scaphoid fractures in wrist injuries, classification systems for these fractures, and the types of surgical approaches for treatment. It emphasizes non-operative and operative management strategies based on fracture stability and displacement. TFCC Repair in 2014: from hammoc to iceberg
TFCC Repair in 2014: from hammoc to icebergNikos Darlis
╠²
This document outlines the classification and management of triangular fibrocartilage complex (TFCC) injuries, including traumatic and degenerative types. It discusses various repair techniques based on the type of TFCC tear and the healing potential associated with acute, subacute, and chronic conditions. The presentation emphasizes tailored approaches for surgical intervention, including arthroscopic methods and ulnar shortening procedures.Radial head fracture
Radial head fractureBahaa Kornah
╠²
The document presents an overview of radial head fractures, including their epidemiology, mechanisms of injury, anatomy, associated injuries, diagnosis, classification, and treatment options. It discusses the importance of identifying related injuries, outlines non-operative and operative management strategies, and compares the outcomes of different surgical interventions. The document highlights the significance of careful evaluation and selection of treatment methods to optimize long-term recovery and function.Talus anatomy, blood supply & fractures
Talus anatomy, blood supply & fracturesHiren Divecha
╠²
This document discusses the anatomy, classification, and management of fractures of the talus bone. It describes the different types of talar fractures including neck, body, lateral and posterior process, and head fractures. It outlines the mechanisms of injury, investigations, treatment options including casting, open reduction internal fixation, and excision depending on the fracture type and degree of displacement. Complications of the different fracture types such as avascular necrosis, osteoarthritis, and malunion are also summarized.Femoro acetabularimpingementsyndrome-130924081558-phpapp02
Femoro acetabularimpingementsyndrome-130924081558-phpapp02Hamid Hejrati
╠²
This document discusses femoro-acetabular impingement (FAI), which occurs when the femoral head and neck abnormally contact the acetabular rim, causing damage. There are two main types: cam impingement from an abnormal femoral head-neck junction; and pincer impingement from acetabular overcoverage. Accurate diagnosis using clinical exams and imaging of the alpha angle and offset ratios is important for determining treatment, which may include hip arthroscopy, osteochondroplasty, or periacetabular osteotomy. FAI is commonly seen in young, active individuals and certain athletic activities increase risk.Scaphoid non unions
Scaphoid non unionsVaikunthan Rajaratnam
╠²
This document reviews scaphoid fractures, including:
- Anatomy, blood supply, biomechanics and kinematics of the scaphoid bone
- Risk factors, classification, investigations and diagnosis of scaphoid fractures
- Treatment options for both acute scaphoid fractures and scaphoid nonunions including nonoperative treatment, operative fixation, bone grafting techniques and outcomes
- Vascularized bone grafting can achieve higher union rates for proximal pole scaphoid nonunions with avascular necrosis compared to non-vascularized grafts.╬ƒ╬¥╬Á╬»╬Á¤é ╬í╬«╬¥╬Á╬╣¤é ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à- Acute TFCC Tears 2015
╬ƒ╬¥╬Á╬»╬Á¤é ╬í╬«╬¥╬Á╬╣¤é ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à- Acute TFCC Tears 2015Nikos Darlis
╠²
This document discusses acute triangular fibrocartilage complex (TFCC) tears. It begins with an overview of TFCC anatomy and Palmer's classification of TFCC tears. For acute TFCC tears associated with distal radius fractures, the document recommends initial conservative treatment for 8-12 weeks. It notes that TFCC tears are commonly seen with distal radius fractures, especially when there is over 5-7mm of shortening, radial displacement of the ulnar styloid base, or over 25-30 degrees of angulation. The treatment algorithm recommends considering arthroscopy for distal radius fractures with TFCC tears or distal radioulnar joint instability. For isolated TFCC tears, conservative treatment is recommended initially. The timing and approach to repair versusArthroscopic treatment of scaphoid fractures & nonunions
Arthroscopic treatment of scaphoid fractures & nonunionsAaron Venouziou
╠²
This document discusses arthroscopic treatment of scaphoid fractures and nonunions. It notes that scaphoid fractures make up 70% of all carpal fractures, most common in males aged 15-30, and are often sports-related injuries. Nonoperative treatment results in healing within 6-8 weeks for undisplaced fractures, but longer for displaced fractures. Operative treatment is recommended for displaced fractures, fractures over 1mm displaced, fractures over 35 degrees angulated, or fractures with associated soft tissue injuries. Arthroscopically assisted percutaneous fixation allows for direct visualization of fracture reduction and guide wire placement, helping ensure central screw placement which results in better fixation and union rates. This technique is described for both acuteHill sachs
Hill sachsRitesh Mahajan
╠²
1. The patient has a history of recurrent anterior dislocations of the right shoulder.
2. MRI of the right shoulder found a 19.5mm exaggerated concavity and thin curvilinear streak of edema on the posterolateral aspect of the humeral head, consistent with a Hill-Sachs lesion.
3. A Hill-Sachs lesion is a compression fracture of the posterolateral humeral head that occurs during anterior shoulder dislocations and results in impaction of the humeral head against the glenoid rim.PELVIC FRACTURES ÔÇô ANATOMY, TYPES, MANAGEMENT &OUTCOME - EVIDENCE BASED ANALYSIS
PELVIC FRACTURES ÔÇô ANATOMY, TYPES, MANAGEMENT &OUTCOME - EVIDENCE BASED ANALYSISanytumour
╠²
This document provides an overview of pelvic fractures, including epidemiology, classification systems, imaging, management, and treatment approaches. It discusses the anatomy of the pelvic ring and mechanisms of injury. Common classification systems like Young-Burgess and Tile are described. Treatment depends on fracture type and stability, ranging from non-operative management to external or internal fixation. Internal fixation techniques are outlined for anterior and posterior ring injuries. Outcomes are often dependent on associated injuries rather than the pelvic fracture itself.Olecranon fracture
Olecranon fractureShalini Devani
╠²
An olecranon fracture is a break of the proximal end of the ulna bone where it forms part of the elbow joint. It most often occurs from a fall on an outstretched arm. Diagnosis is made through physical exam finding tenderness and a gap at the fracture site as well as x-rays. Treatment depends on the severity of the break, with minor fractures treated by casting and more severe displaced fractures requiring surgical fixation such as screws, plates or wires to stabilize the bone fragments. Complications can include stiffness, non-healing of the fracture and arthritis if not properly treated.Blood supply & fractures of scaphoid
Blood supply & fractures of scaphoidorthoprince
╠²
The document discusses the blood supply and anatomy of the scaphoid bone in the wrist. It notes that the scaphoid receives most of its blood supply from the dorsal branches of the radial artery, putting it at high risk for osteonecrosis if fractured. It describes different classification systems for scaphoid fractures and presents options for management, including cast immobilization, percutaneous fixation, open surgery and arthroscopy. Complications of fractures like nonunion are also outlined.Talar fractures2
Talar fractures2Jayant Sharma
╠²
This document discusses fractures of the talus bone in the foot. It begins by describing the talus bone's anatomy and blood supply. It then discusses the different types of talus fractures including fractures of the neck, body, head, and processes. For each fracture type, it covers mechanisms of injury, classification systems, diagnostic imaging, treatment approaches such as casting, open reduction and internal fixation, and potential complications like osteonecrosis and malunion. Throughout, it emphasizes the importance of early and accurate reduction to optimize outcomes given the tenuous blood supply to the talus.Femoroacetabular impingement
Femoroacetabular impingementChrysovergis Chrysovergis
╠²
This document discusses femoro-acetabular impingement (FAI), which occurs when the femoral head and neck abnormally contact the acetabular rim, causing early hip degeneration. FAI has three types based on anatomy: cam, pincer, and mixed. Diagnosis involves clinical exams, x-rays to detect bone abnormalities, and MRI to view soft tissues. Conservative treatment provides temporary relief while surgery corrects the underlying impingement through osteoplasty or labral repair. Both open surgery and hip arthroscopy are effective surgical options for FAI.╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é 016/ Acute DRUJ Instability 016
╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é 016/ Acute DRUJ Instability 016Nikos Darlis
╠²
The document discusses acute distal radioulnar joint (DRUJ) instability, including clinical diagnosis methods and treatment options. It explores the anatomy, mechanics, and common injuries related to DRUJ, specifically focusing on ulnar head dislocations and distal radius fractures. Management strategies for various types of injuries, including conservative and surgical interventions, are summarized along with complications and recovery considerations.Scaphoid fracture and non union
Scaphoid fracture and non unionratish mishra
╠²
The document discusses scaphoid fractures, including:
- Anatomy of the scaphoid bone and its blood supply.
- Mechanisms of injury typically involve falls on an outstretched hand causing hyperextension and radial deviation of the wrist.
- Classification systems for scaphoid fractures include Russe's, Mayo, Herbert's, and AO.
- Treatment depends on fracture displacement and stability, ranging from cast immobilization for nondisplaced fractures to surgery for displaced or unstable fractures.05. clavicle injuries
05. clavicle injuriesFahad Zakwan
╠²
This document reviews injuries to the clavicle, acromioclavicular joint, and sternoclavicular joint. It begins by reviewing the anatomy of these areas. It then discusses imaging and classifications of fractures of the clavicle, injuries to the acromioclavicular joint, and injuries to the sternoclavicular joint. For each type of injury, the document reviews treatment options such as nonoperative treatment versus surgical repair or reconstruction. Complications are also discussed.╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é & ╬í╬«╬¥╬Á╬╣¤é ¤ä╬┐¤à ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à - Acute D...
╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é & ╬í╬«╬¥╬Á╬╣¤é ¤ä╬┐¤à ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à - Acute D...Nikos Darlis
╠²
The document discusses the anatomy and management of the distal radioulnar joint (DRUJ), highlighting congenital and acquired factors affecting stability and dislocation. It details various conditions and injuries related to the forearm and wrist, including cases of TFCC tears, Galeazzi and Essex-Lopresti injuries, and associated fracture patterns. Emphasis is placed on diagnosing stability, treatment options, and the healing potential of different ligaments and tissues in the area.Carpal Fractures
Carpal Fracturesjfreshour
╠²
1. Wilhelm Roentgen discovered x-rays in 1895, allowing for better diagnosis and classification of wrist fractures. Scaphoid fractures are the most common carpal bone fractures, accounting for 70% of carpal fractures.
2. Treatment options depend on the specific bone fractured and degree of displacement. Nondisplaced fractures are usually treated conservatively with casting while displaced fractures often require surgical fixation using methods like K-wire fixation.
3. Complications can include nonunion, pain, and arthritis. However, advances in surgical techniques and hardware have reduced morbidity and allowed for faster rehabilitation, important considerations for athlete patients.Instability around elbow -1st part
Instability around elbow -1st partVishnu Raja
╠²
1) The document discusses various ligaments and structures involved in elbow stability, including the lateral and medial ligamentous complexes.
2) It describes the biomechanics of acute elbow dislocations and different types of elbow instabilities such as posterolateral rotatory instability.
3) Clinical evaluation for elbow instability involves various tests like the lateral pivot shift test and management includes repairing injured ligaments, reconstructing chronic injuries, and addressing any bone deficiencies through procedures like radial head replacement.Management of chronic elbow instability 13
Management of chronic elbow instability 13Omar Elhamroush
╠²
This document discusses the management of chronic elbow instability. It begins by defining the anatomy and stabilizers of the elbow joint. It then describes the different types of elbow instability, including traumatic causes like acute dislocation and chronic lateral/medial instability, as well as non-traumatic causes. Diagnosis involves special tests to assess varus and valgus instability. Treatment depends on the type and chronicity of instability, and may include closed reduction, ligament repair/reconstruction, and external fixation. The goal of treatment is to restore the functional integrity of the medial and lateral collateral ligaments.Talus fructures classification and managment
Talus fructures classification and managment drhakim90
╠²
The document discusses various types of talus fractures, including incidence rates, causes, evaluations, and treatment options. It highlights the importance of anatomical reduction and stable internal fixation to minimize complications such as osteonecrosis and posttraumatic arthritis. Fractures of the talus are relatively uncommon but can have serious implications due to the bone's unique anatomy and blood supply issues.Seminar rotator cuff
Seminar rotator cuffChapma9
╠²
The document summarizes the glenohumeral joint and rotator cuff. It describes the anatomy of the joint and rotator cuff muscles. It then discusses rotator cuff pathology, symptoms, physical exam maneuvers, and special tests to assess the rotator cuff including the empty can test, lift-off test, and external rotation lag sign.Rotator cuff Repair - New Techniques and Challenges
Rotator cuff Repair - New Techniques and ChallengesShoulderPain
╠²
The document discusses advancements and challenges in rotator cuff repair (RCR) techniques, highlighting a potential market expansion as the aging population increases. It emphasizes the importance of various factors such as the surgeon's experience, patient characteristics, and implant techniques on repair outcomes and healing rates. Additionally, it reviews emerging technologies and strategies aimed at improving the mechanical strength and biological environment of rotator cuff repairs.More Related Content
What's hot (20)
Radial head fracture
Radial head fractureBahaa Kornah
╠²
The document presents an overview of radial head fractures, including their epidemiology, mechanisms of injury, anatomy, associated injuries, diagnosis, classification, and treatment options. It discusses the importance of identifying related injuries, outlines non-operative and operative management strategies, and compares the outcomes of different surgical interventions. The document highlights the significance of careful evaluation and selection of treatment methods to optimize long-term recovery and function.Talus anatomy, blood supply & fractures
Talus anatomy, blood supply & fracturesHiren Divecha
╠²
This document discusses the anatomy, classification, and management of fractures of the talus bone. It describes the different types of talar fractures including neck, body, lateral and posterior process, and head fractures. It outlines the mechanisms of injury, investigations, treatment options including casting, open reduction internal fixation, and excision depending on the fracture type and degree of displacement. Complications of the different fracture types such as avascular necrosis, osteoarthritis, and malunion are also summarized.Femoro acetabularimpingementsyndrome-130924081558-phpapp02
Femoro acetabularimpingementsyndrome-130924081558-phpapp02Hamid Hejrati
╠²
This document discusses femoro-acetabular impingement (FAI), which occurs when the femoral head and neck abnormally contact the acetabular rim, causing damage. There are two main types: cam impingement from an abnormal femoral head-neck junction; and pincer impingement from acetabular overcoverage. Accurate diagnosis using clinical exams and imaging of the alpha angle and offset ratios is important for determining treatment, which may include hip arthroscopy, osteochondroplasty, or periacetabular osteotomy. FAI is commonly seen in young, active individuals and certain athletic activities increase risk.Scaphoid non unions
Scaphoid non unionsVaikunthan Rajaratnam
╠²
This document reviews scaphoid fractures, including:
- Anatomy, blood supply, biomechanics and kinematics of the scaphoid bone
- Risk factors, classification, investigations and diagnosis of scaphoid fractures
- Treatment options for both acute scaphoid fractures and scaphoid nonunions including nonoperative treatment, operative fixation, bone grafting techniques and outcomes
- Vascularized bone grafting can achieve higher union rates for proximal pole scaphoid nonunions with avascular necrosis compared to non-vascularized grafts.╬ƒ╬¥╬Á╬»╬Á¤é ╬í╬«╬¥╬Á╬╣¤é ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à- Acute TFCC Tears 2015
╬ƒ╬¥╬Á╬»╬Á¤é ╬í╬«╬¥╬Á╬╣¤é ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à- Acute TFCC Tears 2015Nikos Darlis
╠²
This document discusses acute triangular fibrocartilage complex (TFCC) tears. It begins with an overview of TFCC anatomy and Palmer's classification of TFCC tears. For acute TFCC tears associated with distal radius fractures, the document recommends initial conservative treatment for 8-12 weeks. It notes that TFCC tears are commonly seen with distal radius fractures, especially when there is over 5-7mm of shortening, radial displacement of the ulnar styloid base, or over 25-30 degrees of angulation. The treatment algorithm recommends considering arthroscopy for distal radius fractures with TFCC tears or distal radioulnar joint instability. For isolated TFCC tears, conservative treatment is recommended initially. The timing and approach to repair versusArthroscopic treatment of scaphoid fractures & nonunions
Arthroscopic treatment of scaphoid fractures & nonunionsAaron Venouziou
╠²
This document discusses arthroscopic treatment of scaphoid fractures and nonunions. It notes that scaphoid fractures make up 70% of all carpal fractures, most common in males aged 15-30, and are often sports-related injuries. Nonoperative treatment results in healing within 6-8 weeks for undisplaced fractures, but longer for displaced fractures. Operative treatment is recommended for displaced fractures, fractures over 1mm displaced, fractures over 35 degrees angulated, or fractures with associated soft tissue injuries. Arthroscopically assisted percutaneous fixation allows for direct visualization of fracture reduction and guide wire placement, helping ensure central screw placement which results in better fixation and union rates. This technique is described for both acuteHill sachs
Hill sachsRitesh Mahajan
╠²
1. The patient has a history of recurrent anterior dislocations of the right shoulder.
2. MRI of the right shoulder found a 19.5mm exaggerated concavity and thin curvilinear streak of edema on the posterolateral aspect of the humeral head, consistent with a Hill-Sachs lesion.
3. A Hill-Sachs lesion is a compression fracture of the posterolateral humeral head that occurs during anterior shoulder dislocations and results in impaction of the humeral head against the glenoid rim.PELVIC FRACTURES ÔÇô ANATOMY, TYPES, MANAGEMENT &OUTCOME - EVIDENCE BASED ANALYSIS
PELVIC FRACTURES ÔÇô ANATOMY, TYPES, MANAGEMENT &OUTCOME - EVIDENCE BASED ANALYSISanytumour
╠²
This document provides an overview of pelvic fractures, including epidemiology, classification systems, imaging, management, and treatment approaches. It discusses the anatomy of the pelvic ring and mechanisms of injury. Common classification systems like Young-Burgess and Tile are described. Treatment depends on fracture type and stability, ranging from non-operative management to external or internal fixation. Internal fixation techniques are outlined for anterior and posterior ring injuries. Outcomes are often dependent on associated injuries rather than the pelvic fracture itself.Olecranon fracture
Olecranon fractureShalini Devani
╠²
An olecranon fracture is a break of the proximal end of the ulna bone where it forms part of the elbow joint. It most often occurs from a fall on an outstretched arm. Diagnosis is made through physical exam finding tenderness and a gap at the fracture site as well as x-rays. Treatment depends on the severity of the break, with minor fractures treated by casting and more severe displaced fractures requiring surgical fixation such as screws, plates or wires to stabilize the bone fragments. Complications can include stiffness, non-healing of the fracture and arthritis if not properly treated.Blood supply & fractures of scaphoid
Blood supply & fractures of scaphoidorthoprince
╠²
The document discusses the blood supply and anatomy of the scaphoid bone in the wrist. It notes that the scaphoid receives most of its blood supply from the dorsal branches of the radial artery, putting it at high risk for osteonecrosis if fractured. It describes different classification systems for scaphoid fractures and presents options for management, including cast immobilization, percutaneous fixation, open surgery and arthroscopy. Complications of fractures like nonunion are also outlined.Talar fractures2
Talar fractures2Jayant Sharma
╠²
This document discusses fractures of the talus bone in the foot. It begins by describing the talus bone's anatomy and blood supply. It then discusses the different types of talus fractures including fractures of the neck, body, head, and processes. For each fracture type, it covers mechanisms of injury, classification systems, diagnostic imaging, treatment approaches such as casting, open reduction and internal fixation, and potential complications like osteonecrosis and malunion. Throughout, it emphasizes the importance of early and accurate reduction to optimize outcomes given the tenuous blood supply to the talus.Femoroacetabular impingement
Femoroacetabular impingementChrysovergis Chrysovergis
╠²
This document discusses femoro-acetabular impingement (FAI), which occurs when the femoral head and neck abnormally contact the acetabular rim, causing early hip degeneration. FAI has three types based on anatomy: cam, pincer, and mixed. Diagnosis involves clinical exams, x-rays to detect bone abnormalities, and MRI to view soft tissues. Conservative treatment provides temporary relief while surgery corrects the underlying impingement through osteoplasty or labral repair. Both open surgery and hip arthroscopy are effective surgical options for FAI.╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é 016/ Acute DRUJ Instability 016
╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é 016/ Acute DRUJ Instability 016Nikos Darlis
╠²
The document discusses acute distal radioulnar joint (DRUJ) instability, including clinical diagnosis methods and treatment options. It explores the anatomy, mechanics, and common injuries related to DRUJ, specifically focusing on ulnar head dislocations and distal radius fractures. Management strategies for various types of injuries, including conservative and surgical interventions, are summarized along with complications and recovery considerations.Scaphoid fracture and non union
Scaphoid fracture and non unionratish mishra
╠²
The document discusses scaphoid fractures, including:
- Anatomy of the scaphoid bone and its blood supply.
- Mechanisms of injury typically involve falls on an outstretched hand causing hyperextension and radial deviation of the wrist.
- Classification systems for scaphoid fractures include Russe's, Mayo, Herbert's, and AO.
- Treatment depends on fracture displacement and stability, ranging from cast immobilization for nondisplaced fractures to surgery for displaced or unstable fractures.05. clavicle injuries
05. clavicle injuriesFahad Zakwan
╠²
This document reviews injuries to the clavicle, acromioclavicular joint, and sternoclavicular joint. It begins by reviewing the anatomy of these areas. It then discusses imaging and classifications of fractures of the clavicle, injuries to the acromioclavicular joint, and injuries to the sternoclavicular joint. For each type of injury, the document reviews treatment options such as nonoperative treatment versus surgical repair or reconstruction. Complications are also discussed.╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é & ╬í╬«╬¥╬Á╬╣¤é ¤ä╬┐¤à ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à - Acute D...
╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é & ╬í╬«╬¥╬Á╬╣¤é ¤ä╬┐¤à ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à - Acute D...Nikos Darlis
╠²
The document discusses the anatomy and management of the distal radioulnar joint (DRUJ), highlighting congenital and acquired factors affecting stability and dislocation. It details various conditions and injuries related to the forearm and wrist, including cases of TFCC tears, Galeazzi and Essex-Lopresti injuries, and associated fracture patterns. Emphasis is placed on diagnosing stability, treatment options, and the healing potential of different ligaments and tissues in the area.Carpal Fractures
Carpal Fracturesjfreshour
╠²
1. Wilhelm Roentgen discovered x-rays in 1895, allowing for better diagnosis and classification of wrist fractures. Scaphoid fractures are the most common carpal bone fractures, accounting for 70% of carpal fractures.
2. Treatment options depend on the specific bone fractured and degree of displacement. Nondisplaced fractures are usually treated conservatively with casting while displaced fractures often require surgical fixation using methods like K-wire fixation.
3. Complications can include nonunion, pain, and arthritis. However, advances in surgical techniques and hardware have reduced morbidity and allowed for faster rehabilitation, important considerations for athlete patients.Instability around elbow -1st part
Instability around elbow -1st partVishnu Raja
╠²
1) The document discusses various ligaments and structures involved in elbow stability, including the lateral and medial ligamentous complexes.
2) It describes the biomechanics of acute elbow dislocations and different types of elbow instabilities such as posterolateral rotatory instability.
3) Clinical evaluation for elbow instability involves various tests like the lateral pivot shift test and management includes repairing injured ligaments, reconstructing chronic injuries, and addressing any bone deficiencies through procedures like radial head replacement.Management of chronic elbow instability 13
Management of chronic elbow instability 13Omar Elhamroush
╠²
This document discusses the management of chronic elbow instability. It begins by defining the anatomy and stabilizers of the elbow joint. It then describes the different types of elbow instability, including traumatic causes like acute dislocation and chronic lateral/medial instability, as well as non-traumatic causes. Diagnosis involves special tests to assess varus and valgus instability. Treatment depends on the type and chronicity of instability, and may include closed reduction, ligament repair/reconstruction, and external fixation. The goal of treatment is to restore the functional integrity of the medial and lateral collateral ligaments.Talus fructures classification and managment
Talus fructures classification and managment drhakim90
╠²
The document discusses various types of talus fractures, including incidence rates, causes, evaluations, and treatment options. It highlights the importance of anatomical reduction and stable internal fixation to minimize complications such as osteonecrosis and posttraumatic arthritis. Fractures of the talus are relatively uncommon but can have serious implications due to the bone's unique anatomy and blood supply issues.╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é 016/ Acute DRUJ Instability 016
╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é 016/ Acute DRUJ Instability 016Nikos Darlis
╠²
╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é & ╬í╬«╬¥╬Á╬╣¤é ¤ä╬┐¤à ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à - Acute D...
╬ƒ╬¥╬Á╬»╬▒ ╬æ¤â¤ä╬¼╬©╬Á╬╣╬▒ ¤ä╬À¤é ╬å¤Ç¤ë ╬Ü╬Á¤ü╬║╬╣╬┤¤ë╬╗╬Á╬¢╬╣╬║╬«¤é & ╬í╬«╬¥╬Á╬╣¤é ¤ä╬┐¤à ╬ñ¤ü╬»╬│¤ë╬¢╬┐¤à ╬º¤î╬¢╬┤¤ü╬┐¤à - Acute D...Nikos Darlis
╠²
Viewers also liked (11)
Seminar rotator cuff
Seminar rotator cuffChapma9
╠²
The document summarizes the glenohumeral joint and rotator cuff. It describes the anatomy of the joint and rotator cuff muscles. It then discusses rotator cuff pathology, symptoms, physical exam maneuvers, and special tests to assess the rotator cuff including the empty can test, lift-off test, and external rotation lag sign.Rotator cuff Repair - New Techniques and Challenges
Rotator cuff Repair - New Techniques and ChallengesShoulderPain
╠²
The document discusses advancements and challenges in rotator cuff repair (RCR) techniques, highlighting a potential market expansion as the aging population increases. It emphasizes the importance of various factors such as the surgeon's experience, patient characteristics, and implant techniques on repair outcomes and healing rates. Additionally, it reviews emerging technologies and strategies aimed at improving the mechanical strength and biological environment of rotator cuff repairs.Rotator cuff
Rotator cuffAdnan Rashid, MD
╠²
1) A 34-year-old male presented with left shoulder pain and weakness after a fall from his bike three months prior. X-rays after the injury were normal.
2) Ultrasound of the shoulder revealed a rupture of the supraspinatus tendon, which was supported by subsequent MRI findings.
3) Ultrasound is a highly accurate, cost-effective first-line imaging method for evaluating rotator cuff injuries like tendon ruptures, though it requires an experienced sonographer due to some technical challenges. MRI and MR arthrography can also accurately diagnose full and partial thickness tears but are more expensive and involve radiation with some techniques.Rotator cuff disorder
Rotator cuff disorderAlAhly sporting club
╠²
This document describes the anatomy and function of the rotator cuff muscles, as well as causes, diagnosis, and treatment of rotator cuff injuries. It notes that the rotator cuff is comprised of 4 muscles that stabilize the shoulder joint. Rotator cuff injuries can range from inflammation to complete tears and are usually caused by overuse, aging, or trauma. Treatment involves rest, anti-inflammatories, cortisone injections, and physical therapy, with surgery reserved for tears not improving otherwise.Rotator cuff injuries
Rotator cuff injuriesorthoprince
╠²
Rotator cuff injuries can occur due to overuse, trauma, or age-related degeneration. Common causes include repetitive overhead activities in sports or occupations. Symptoms include shoulder pain that is worsened by movement. Diagnosis involves physical examination and may include imaging tests like MRI. Treatment ranges from rest, ice, and anti-inflammatories for mild cases to surgery to repair torn tendons in more severe cases. Rehabilitation focuses on restoring range of motion and strength through a progressive series of exercises.Shoulder dislocation Saseendar
Shoulder dislocation SaseendarDr Saseendar MD
╠²
This document discusses shoulder dislocations, detailing the types (anterior, posterior, inferior), mechanisms, clinical evaluation, and management strategies. It highlights the importance of timely reduction to prevent complications like avascular necrosis and outlines both conservative and operative treatment options for recurrent instability. The content serves as an educational resource for orthopaedic surgery students and emphasizes the need for professional consultation in patient management.Rotator cuff Tear and its management
Rotator cuff Tear and its managementRohan Vakta
╠²
The document discusses rotator cuff tears, including their anatomy, etiology, pathophysiology, and the diagnostic approach. Treatment options range from conservative methods such as physical therapy to surgical interventions like open or arthroscopic repair, each with specific indications and techniques. It emphasizes the importance of timely intervention to prevent muscle atrophy and irreversible damage, potentially leading to significant functional impairment.Shoulder impingement syndrome
Shoulder impingement syndromeRatan Khuman
╠²
This document discusses shoulder impingement syndrome, including its anatomy, causes, symptoms, diagnosis, stages, and treatment approaches. It provides details on the rotator cuff muscles, signs and symptoms of impingement, external and internal factors that can lead to impingement, stages of the syndrome, common tests used for diagnosis, goals of treatment, and manual therapy, therapeutic exercise, and preventative measures used in treatment.Rotator cuff tears
Rotator cuff tearsPaudel Sushil
╠²
This document provides a review of rotator cuff tears, including their anatomy, function, pathophysiology, clinical presentation, diagnostic tests, differential diagnosis, imaging, and treatment options. It describes the rotator cuff muscles and their role in stabilizing the shoulder joint. Common causes of tears include repeated impingement against bony structures or age-related degeneration. Clinical exams aim to isolate each muscle while imaging such as MRI can determine the size and location of tears. Conservative treatment includes corticosteroid injections and physical therapy, while surgical repair is considered for larger or symptomatic tears.Rotator cuff injuries
Rotator cuff injuriesrajusvmc
╠²
This document discusses the anatomy, biomechanics, causes, symptoms, diagnosis, and treatment of rotator cuff tears. It begins by introducing the rotator cuff muscles and their function in stabilizing the shoulder joint. Common causes of tears include impingement, trauma, aging, and ischemia. Symptoms include shoulder pain that is worsened with overhead activities. Diagnosis involves physical exam maneuvers like the Neer's and Hawkins tests as well as imaging like x-rays, ultrasound, CT, or MRI. Treatment ranges from rest, physical therapy, and injections for mild cases to surgical repair for larger or chronic tears if conservative measures fail.Shoulder dislocation Co Norbert
Shoulder dislocation Co Norbert Icyizanye Norbert
╠²
Shoulder dislocation occurs when the head of the humerus separates from the glenoid cavity of the scapula. The glenohumeral joint is a ball-and-socket synovial joint surrounded by ligaments and muscles like the rotator cuff. Anterior dislocation is the most common type, occurring when the arm is abducted, externally rotated, and extended. Physical exam findings include loss of the normal shoulder contour and tenderness. Imaging like x-rays can confirm the diagnosis by showing the humeral head is no longer centered in the glenoid.Ad
Similar to Claviclefrctures (20)
Fracture of Shoulder and Humerus
Fracture of Shoulder and HumerusEneutron
╠²
This document discusses injuries to the shoulder girdle and humerus, including acromioclavicular injuries, dislocations, and fractures of the clavicle. It describes the mechanisms of various injuries, methods of diagnosis including physical exam findings and x-rays, and approaches to treatment including closed reduction techniques and immobilization methods. Reduction methods like Kocher's are outlined step-by-step for anterior shoulder dislocations. Greenstick fractures are noted as common in children. Immobilization with a sling or ring method is generally recommended for clavicle fractures and injuries requiring support.Humeral fractures 1 5 15 aseh
Humeral fractures 1 5 15 asehBrian Daubs
╠²
This document discusses humeral fractures in animals. It describes the causes, types, and treatment of humeral fractures. Most humeral fractures are caused by minor trauma from falls or playing. Distal humeral fractures, which involve the elbow joint, account for about half of all humeral fractures. The lateral humeral condyle is most commonly fractured due to the force from the radial head during weight bearing. Fixation methods for lateral condylar fractures include lag screws or self-compressing orthofix pins. A study found that while both methods provided adequate stability, lag screws generated greater compression over a larger area of the fracture site compared to pins.Fracture of Femur
Fracture of FemurEneutron
╠²
Fractures of the femur, especially the femoral shaft, are among the most common fractures seen by orthopedists, with an incidence of 1.33 fractures per 10,000 people in the United States. Proximal femoral fractures, which include femoral neck, trochanteric, and subtrochanteric fractures, require careful classification to determine appropriate treatment. Surgical fixation is generally preferred but conservative treatment with traction may be used in some cases. Complications can include avascular necrosis, non-union, and osteoarthritis.Biomechanics of Cervical Disk Replacement
Biomechanics of Cervical Disk ReplacementAlexander Bardis
╠²
The document discusses cervical disk replacement and associated biomechanics, emphasizing its rapid growth as a vital spinal surgery procedure. It details various techniques and the development of new implants, indicating promising early results from current studies. Key mechanical performance metrics are outlined, highlighting the importance of durability, motion range, and stability to ensure successful outcomes in cervical disk replacements.Radial artery
Radial arteryDr Ashish gaur
╠²
The document discusses minimally invasive radial artery harvesting techniques. It notes that while initially abandoned due to spasms and poor results, the radial artery is now commonly used as a graft due to improved harvesting methods. Key points discussed include using small incisions, minimal handling of the artery, and applying warm papaverine to prevent spasms. The modified Allen's test and Doppler ultrasound are recommended to confirm hand circulation before harvesting. With minimal handling and spasm prevention, radial arteries can be harvested with low complication rates and good long-term patency for coronary artery bypass grafting.Avn hip
Avn hipDr Imran Jan
╠²
This document discusses surgical procedures for osteonecrosis of the femoral head, including both joint preserving and replacing options. Key joint preserving procedures described are core decompression, various bone grafting techniques using vascularized and nonvascularized grafts, and proximal femoral osteotomies. Total hip arthroplasty and hip resurfacing are mentioned as joint replacing options.howtodotensionbandwire-160809071243.pdf
howtodotensionbandwire-160809071243.pdfdocshahir
╠²
This document provides guidance on performing tension band wiring for patellar fractures. It discusses relevant anatomy, preoperative preparation including imaging and diagnosis, surgical approach and technique, and post-operative care. The surgical technique involves exposing the fracture through a midline incision, reducing fragments with K-wires or forceps, inserting two parallel K-wires outside-in or inside-out, and passing a figure-of-eight tension band wire around the K-wires while tightly twisting the ends. Early range of motion exercises are encouraged post-operatively while wearing a knee splint to allow full weight bearing.How to do tension band wire
How to do tension band wireKhadijah Nordin
╠²
This document provides guidance on performing tension band wiring for patellar fractures. It discusses relevant anatomy, preoperative preparation including imaging and diagnosis, surgical approach and technique, and post-operative care. The surgical technique involves exposing the fracture through a midline incision, reducing fragments with K-wires or forceps, inserting two parallel K-wires outside-in or inside-out, and passing a figure-of-eight tension band wire around the K-wires while tightly twisting the ends. Early range of motion exercises are encouraged post-operatively while wearing a knee splint to regain quadriceps strength before full weight bearing.Shoulder impingement syndrome
Shoulder impingement syndromeHardev Singh
╠²
1) Shoulder impingement syndrome is caused by compression of the rotator cuff tendons between the acromion and humeral head. It commonly results from a hooked acromion or inflammation/thickening of the tendons.
2) Treatment begins conservatively with anti-inflammatories, cortisone injections, and physical therapy. If unsuccessful, surgery such as open or arthroscopic acromioplasty is recommended to remove bone spurs and widen the space.
3) Acromioplasty involves detaching the deltoid muscle, removing the coracoacromial ligament and anterior portion of the acromion, and inspecting/repairing any rotatorTracheostomy
TracheostomySanjay Kumar Kulchania
╠²
This document discusses tracheostomy, which is a surgical procedure that creates an opening in the trachea. It describes the anatomy of the trachea and indications for tracheostomy including upper airway obstruction, pulmonary ventilation, pulmonary toilet, and elective procedures. The document outlines different types of tracheostomy procedures and their techniques, as well as potential complications. It also discusses problems that can occur with tracheostomy care and home care plans.╬Á╬¥╬Á╬╗╬»╬¥╬Á╬╣¤é ¤â¤ä╬À╬¢ ╬▒¤ü╬©¤ü╬┐¤â╬║╬┐¤Ç╬╣╬║╬« ¤ç╬Á╬╣¤ü╬┐¤à¤ü╬│╬╣╬║╬« ¤ä╬À¤é ╬▒╬║¤ü¤ë╬╝╬╣╬┐╬║╬╗╬Á╬╣╬┤╬╣╬║╬«¤é
╬Á╬¥╬Á╬╗╬»╬¥╬Á╬╣¤é ¤â¤ä╬À╬¢ ╬▒¤ü╬©¤ü╬┐¤â╬║╬┐¤Ç╬╣╬║╬« ¤ç╬Á╬╣¤ü╬┐¤à¤ü╬│╬╣╬║╬« ¤ä╬À¤é ╬▒╬║¤ü¤ë╬╝╬╣╬┐╬║╬╗╬Á╬╣╬┤╬╣╬║╬«¤éShoulder Library
╠²
This document discusses advances in arthroscopy of the acromioclavicular (AC) joint. It describes the anatomy of the AC joint and common pathologies like osteolysis, arthritis, cysts, and dislocations that can be treated arthroscopically. Techniques for arthroscopic distal clavicle excision, AC joint reconstruction for dislocations using grafts or ligament transfers are presented. The author's preference is for open reduction and fixation for AC dislocations due to more precise reduction and residual scarring's effect on stability. Several case examples are provided.Fracture of Distal End Humerus.
Fracture of Distal End Humerus.Dr.Anshu Sharma
╠²
Distal humerus fractures, accounting for about 2% of all fractures in adults, involve complex anatomy with critical articular surfaces, requiring careful evaluation via radiographs and potentially CT scans for surgical planning. Supracondylar humerus fractures are the most common in children and predominantly result from falls on outstretched hands, necessitating varying treatment strategies based on fracture types. Complications include nerve injuries and malunion, with nonoperative methods indicated for specific cases, particularly involving elderly patients with significant comorbidities.ACL INJURIES
ACL INJURIESSidheshwar Thosar
╠²
This document provides an overview of anterior cruciate ligament (ACL) injuries, including:
1) The anatomy, functions, and mechanisms of ACL injury. Common symptoms include the knee popping out and difficulty walking. Physical exams include the anterior drawer test and Lachman's test.
2) MRI is the best imaging method, showing primary signs like an absent ACL or secondary signs like bone bruises.
3) Treatment options include non-operative management for mild injuries or reconstruction using autografts like the patellar tendon or hamstring tendons. Proper technique and rehabilitation are important for success.
4) Complications can include limited motion, pain, and failure, which may be due toAnkle fractures
Ankle fracturesDr.Anshu Sharma
╠²
Ankle fractures are common injuries that require careful evaluation to identify bony and soft tissue damage. The ankle is a complex hinge joint supported by ligaments and the tibia, fibula, talus, and deltoid ligament. Classification systems like Lauge-Hansen and Weber are used to characterize fracture patterns and guide management, which may involve closed treatment for stable injuries or surgery to restore ankle anatomy and stability for unstable fractures. Radiographs are important for diagnosis but CT or MRI may be needed to fully evaluate injury extent.Ankle fractures
Ankle fracturesDr.Anshu Sharma
╠²
Ankle fractures are common injuries that require careful evaluation to identify bony and soft tissue damage. The ankle is a complex hinge joint supported by ligaments and the tibia, fibula, talus, and deltoid ligament. Classification systems like Lauge-Hansen and Weber are used to characterize fracture patterns and guide treatment, which may involve closed management or surgery to restore ankle anatomy and stability. Restoring length and rotation of the fibula as well as stabilizing potential syndesmotic injuries is important for successful outcomes.Sacral fractures
Sacral fractures Dibyendunarayan Bid
╠²
Sacral fractures can result from a blow to the tailbone area from a fall. Women are more commonly affected than men. Physical examination may reveal bruising and tenderness over the sacrum or coccyx. X-rays sometimes do not show fractures if they are minor. More serious fractures are classified by Denis zones, with zone III fractures through the sacral body posing the highest risk of neurological injuries like loss of bladder control. Treatment depends on fracture stability and neurological involvement, ranging from rest and cushioning to sacral laminectomy or open reduction and internal fixation. Coccyx fractures from falls also cause severe pain but generally require only analgesics and cushioning.Orthopaedic trauma
Orthopaedic trauma Oryza Satria
╠²
1. Bone is composed of cortical and cancellous bone, with cells including osteoblasts, osteoclasts, and osteoprogenitors. Bone remodeling occurs through the actions of osteoblasts and osteoclasts.
2. There are two types of bone formation: endochondral ossification and intramembranous ossification. Fractures can be classified based on location, displacement, and whether the skin is broken (open vs closed fracture).
3. Fracture healing consists of hematoma, proliferation, callus formation, and remodeling phases. Treatment depends on fracture type and may include splinting, casting, traction, closed or open reduction, and internal or external fixation. Management ofCongenital Deformities
Congenital DeformitiesEneutron
╠²
This document provides information on congenital muscular torticollis and its treatment. It describes how congenital muscular torticollis is caused by fibromatosis in the sternocleidomastoid muscle. Conservative treatment including stretching is recommended during infancy. Surgery may be needed if deformity persists beyond age 1. The goal of surgery before age 6-8 is to allow remodeling and prevent facial asymmetry.Rotatory cuff syndrome & Scapular Dyskinesia
Rotatory cuff syndrome & Scapular DyskinesiaDr. Manoj Parida
╠²
This document discusses scapular dyskinesis and rotator cuff syndrome. It defines scapular dyskinesis as an alteration in the normal position or motion of the scapula during shoulder movements. Scapular dyskinesis is associated with rotator cuff problems and glenohumeral instability. It also presents various tests to identify scapular dyskinesis such as the scapular assistance test. The document then discusses rotator cuff syndrome, defining it as disorders of the rotator cuff muscles including tears, impingement, and tendinitis. It describes the anatomy of the rotator cuff and various classifications of tears.╬Á╬¥╬Á╬╗╬»╬¥╬Á╬╣¤é ¤â¤ä╬À╬¢ ╬▒¤ü╬©¤ü╬┐¤â╬║╬┐¤Ç╬╣╬║╬« ¤ç╬Á╬╣¤ü╬┐¤à¤ü╬│╬╣╬║╬« ¤ä╬À¤é ╬▒╬║¤ü¤ë╬╝╬╣╬┐╬║╬╗╬Á╬╣╬┤╬╣╬║╬«¤é
╬Á╬¥╬Á╬╗╬»╬¥╬Á╬╣¤é ¤â¤ä╬À╬¢ ╬▒¤ü╬©¤ü╬┐¤â╬║╬┐¤Ç╬╣╬║╬« ¤ç╬Á╬╣¤ü╬┐¤à¤ü╬│╬╣╬║╬« ¤ä╬À¤é ╬▒╬║¤ü¤ë╬╝╬╣╬┐╬║╬╗╬Á╬╣╬┤╬╣╬║╬«¤éShoulder Library
╠²
Ad
Claviclefrctures
- 1. ClavicularClavicular fracturesfractures Dr. Rutuj KamdarDr. Rutuj Kamdar SIORSIOR
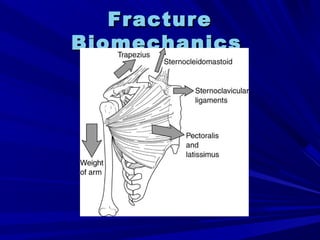
- 2. Relevant anatomyRelevant anatomy Weakest part is where change of curvatureWeakest part is where change of curvature occursoccurs the superomedialthe superomedial clavicleclavicle serves as an origin ofserves as an origin of the sternocleidomastoid. In a midshaftthe sternocleidomastoid. In a midshaft clavicleclavicle fracture, the sternocleidomastoid elevates thefracture, the sternocleidomastoid elevates the medial fragmentmedial fragment Anterior to the clavicleAnterior to the clavicle lie the supraclavicularlie the supraclavicular nervesnerves
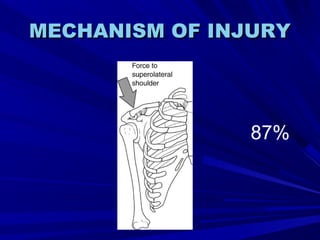
- 4. MECHANISM OF INJURYMECHANISM OF INJURY 87%
- 6. CLASSIFICATIONSCLASSIFICATIONS Possibly the most commonly used systemPossibly the most commonly used system is that of Allman .He separatedis that of Allman .He separated clavicleclavicle fractures into three groups:fractures into three groups: Group IÔÇömiddle third fracturesGroup IÔÇömiddle third fractures Group IIÔÇölateral third fracturesGroup IIÔÇölateral third fractures Group IIIÔÇömedial third fracturesGroup IIIÔÇömedial third fractures
- 9. RELATIVE INCIDENCESRELATIVE INCIDENCES MIDSHAFT FRACTURES MOST COMMONMIDSHAFT FRACTURES MOST COMMON MEDIAL FRACTURES RAREMEDIAL FRACTURES RARE The medialThe medial clavicleclavicle is also the most frequentis also the most frequent site of pathologic fracture, owing to its proximitysite of pathologic fracture, owing to its proximity to the head and neck. In cases of fractureto the head and neck. In cases of fracture displacement combined with spinal accessorydisplacement combined with spinal accessory palsy, operative fixation of thepalsy, operative fixation of the clavicle shouldclavicle should be consideredbe considered
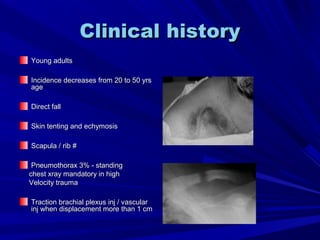
- 10. Clinical historyClinical history Young adultsYoung adults Incidence decreases from 20 to 50 yrsIncidence decreases from 20 to 50 yrs ageage Direct fallDirect fall Skin tenting and echymosisSkin tenting and echymosis Scapula / rib #Scapula / rib # Pneumothorax 3% - standingPneumothorax 3% - standing chest xray mandatory in highchest xray mandatory in high Velocity traumaVelocity trauma Traction brachial plexus inj / vascularTraction brachial plexus inj / vascular inj when displacement more than 1 cminj when displacement more than 1 cm
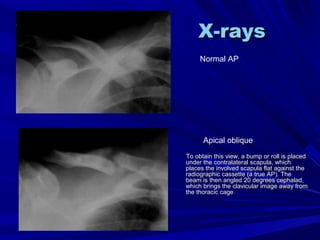
- 11. X-raysX-rays To obtain this view, a bump or roll is placedTo obtain this view, a bump or roll is placed under the contralateral scapula, whichunder the contralateral scapula, which places the involved scapula flat against theplaces the involved scapula flat against the radiographic cassette (a true AP). Theradiographic cassette (a true AP). The beam is then angled 20 degrees cephalad,beam is then angled 20 degrees cephalad, which brings the clavicular image away fromwhich brings the clavicular image away from the thoracic cagethe thoracic cage Normal AP Apical oblique
- 12. Other XRAYSOther XRAYS For lateral fractures, a 10-pound stressFor lateral fractures, a 10-pound stress view to analyze for integrity of theview to analyze for integrity of the coracoclavicular ligaments may becoracoclavicular ligaments may be necessary.necessary. For intraarticular fractures of theFor intraarticular fractures of the acromioclavicular joint, an axillaryacromioclavicular joint, an axillary radiograph or Zanca 15-degree apicalradiograph or Zanca 15-degree apical oblique view of the shoulder may be usefuloblique view of the shoulder may be useful
- 13. TREATMENT : MEDIALTREATMENT : MEDIAL 1/3RD1/3RD CONSERVATIVECONSERVATIVE OPERATIVE IF PATHOLOGICALOPERATIVE IF PATHOLOGICAL FRACTUREFRACTURE
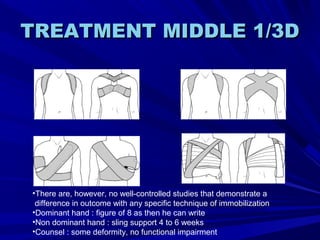
- 14. TREATMENT MIDDLE 1/3DTREATMENT MIDDLE 1/3D ÔÇóThere are, however, no well-controlled studies that demonstrate a difference in outcome with any specific technique of immobilization ÔÇóDominant hand : figure of 8 as then he can write ÔÇóNon dominant hand : sling support 4 to 6 weeks ÔÇóCounsel : some deformity, no functional impairment
- 15. CLOSED REDUCTIONCLOSED REDUCTION In the supine technique, a pillow is placedIn the supine technique, a pillow is placed between the scapulae while the shoulders arebetween the scapulae while the shoulders are manipulated superiorly and laterally (35,159). Inmanipulated superiorly and laterally (35,159). In the sitting technique, a knee is placed betweenthe sitting technique, a knee is placed between the scapulae and a sheet is used, in athe scapulae and a sheet is used, in a configuration similar to a figure-of-eightconfiguration similar to a figure-of-eight bandage, to pull the scapulae outward. The usebandage, to pull the scapulae outward. The use of a hematoma block aids in the techniqueof a hematoma block aids in the technique
- 16. OPERATIVE TREATMENTOPERATIVE TREATMENT CLOSED REDUCTIONCLOSED REDUCTION INTRAMEDULLARY PINS OR WIREINTRAMEDULLARY PINS OR WIRE OPEN REDUCTION AND FIXATIONOPEN REDUCTION AND FIXATION WITH A PLATE ( PLATE FELTWITH A PLATE ( PLATE FELT SUBCUTANEOUSLY)SUBCUTANEOUSLY)
- 18. LATERAL 3LATERAL 3RDRD FRACTURESFRACTURES Type I and type III distal clavicleType I and type III distal clavicle fractures are treated nonoperativelyfractures are treated nonoperatively Both groups, but particularly those withBoth groups, but particularly those with type III injuries, are warned of thetype III injuries, are warned of the possibility of late acromioclavicularpossibility of late acromioclavicular arthrosis with the possible need forarthrosis with the possible need for subsequent distal clavicle excisionsubsequent distal clavicle excision
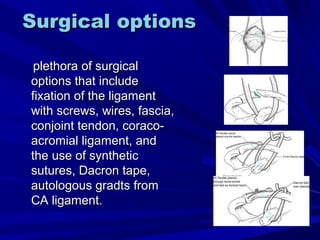
- 19. Surgical optionsSurgical options plethora of surgicalplethora of surgical options that includeoptions that include fixation of the ligamentfixation of the ligament with screws, wires, fascia,with screws, wires, fascia, conjoint tendon, coraco-conjoint tendon, coraco- acromial ligament, andacromial ligament, and the use of syntheticthe use of synthetic sutures, Dacron tape,sutures, Dacron tape, autologous gradts fromautologous gradts from CA ligament.CA ligament.
- 21. Complications of # clavicleComplications of # clavicle MalunuionMalunuion Non unionNon union Brachial plexus traction injuriesBrachial plexus traction injuries Post traumatic arthritisPost traumatic arthritis
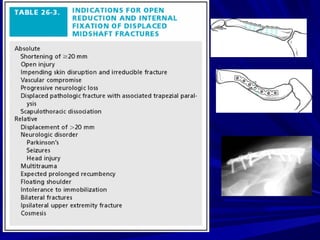
- 22. ConclusionConclusion Clavicle fractures usually heal uneventfully, even in theClavicle fractures usually heal uneventfully, even in the presence of treatment noncompliance.presence of treatment noncompliance. For most of these fractures, initial patient counseling asFor most of these fractures, initial patient counseling as to the expected result is probably the most importantto the expected result is probably the most important aspect of treatment.aspect of treatment. In contrast, certain fracture types, such as the displacedIn contrast, certain fracture types, such as the displaced and shortened midshaft fracture or the type II distaland shortened midshaft fracture or the type II distal clavicle fracture, require special attention. Whenclavicle fracture, require special attention. When necessary, operative intervention should be based onnecessary, operative intervention should be based on counterbalancing the deforming forces, specifically thecounterbalancing the deforming forces, specifically the weight of the arm. In the face of symptomatic nonunion,weight of the arm. In the face of symptomatic nonunion, bone grafting and plate fixation is an effective option.bone grafting and plate fixation is an effective option.
- 23. BibliographyBibliography Rockwood and GreenRockwood and Green internetinternet