Cme expenses format
?Download as DOCX, PDF?
0 likes?242 views

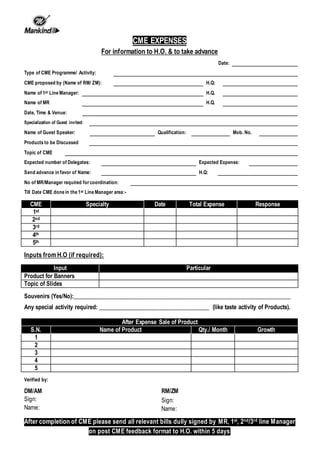
This document outlines the details required for a continuing medical education (CME) program, including the type of program, speaker information, topic, expected attendees and expenses. It requests an advance payment be sent to the specified individual and lists the prior CME events done in the manager's area. Input from headquarters is sought on banners, slides or souvenirs. Product sales metrics before and after the CME are to be tracked and the completed form with bills signed by managers must be returned within 5 days.
Cme expenses format
- 1. CME EXPENSES For information to H.O. & to take advance Date: Type of CME Programme/ Activity: CME proposed by (Name of RM/ ZM): H.Q: Name of 1st Line Manager: H.Q. Name of MR H.Q. Date, Time & Venue: Specialization of Guest invited: Name of Guest Speaker: Qualification: Mob. No. Products to be Discussed Topic of CME Expected number of Delegates: Expected Expense: Send advance in favor of Name: H.Q: No of MR/Manager required for coordination: Till Date CME done in the 1st Line Manager area:- CME Specialty Date Total Expense Response 1st 2nd 3rd 4th 5th Inputs from H.O (if required): Input Particular Product for Banners Topic of ∫›∫›fl£s Souvenirs (Yes/No):__________________________________________________________________________ Any special activity required: ______________________________________ (like taste activity of Products). After Expense Sale of Product S.N. Name of Product Qty./ Month Growth 1 2 3 4 5 Verified by: DM/AM RM/ZM Sign: Sign: Name: Name: After completion of CME please send all relevant bills dully signed by MR, 1st, 2nd/3rd line Manager on post CME feedback format to H.O. within 5 days