Common peroneal nerve lesions
•Download as PPTX, PDF•
25 likes•23,513 views

Common peroneal nerve lesions often present with foot drop and loss of sensation in the lower leg and foot. The common peroneal nerve is susceptible to injury where it passes between muscles in the leg and around the fibula bone. Injuries can occur from trauma, fractures, compression, ischemia or tight footwear and result in weakness of ankle dorsiflexion. Physical exams may show reduced foot movement and sensation loss while nerve conduction studies can identify injuries. Treatment focuses on bracing, stimulation, positioning and protective devices to prevent foot drop and sprains.

Common peroneal nerve lesions
- 1. COMMON PERONEAL NERVE LESIONS Presented by Louis law Mwadziwana
- 2. ď‚ž Common peroneal neuropathy is the most common mononeuropathy encountered in the lower limb. ď‚ž Weakness of ankle dorsiflexion and the resultant foot drop are common presentations. ď‚ž It may also present with loss of sensation limited to the distribution of the deep or superficial peroneal nerve or its branches
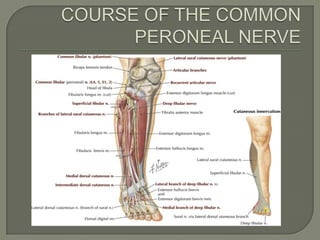
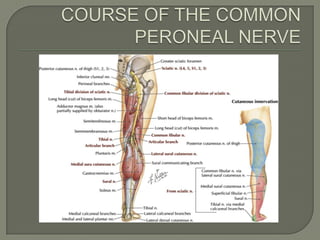
- 3. The common peroneal nerve is closely related to the head and neck of the fibular. ď‚ž The nerve passes between the two heads of the peroneus longus where it is flattened and its constituent bundles are separated so that the nutrient vessels are exposed and are left unprotected between them. ď‚ž It then curves round the neck of the fibula and then divide into its deep and superficial divisions. ď‚ž Just before the nerve enters the peroneus longus it is held applied to bone and muscle attachments of the deep fascia. Not only is the nerve fixed at this point it is also angulated where it turns abruptly laterally from the gastrocnemius to pass between the two heads of the peroneus longus. ď‚ž
- 6. ď‚ž The above anatomical features render the nerve and its nutrient vessels susceptible to damage in injuries about the knee.
- 7.  Traction • By posterior dislocation of the tibio-fibular joint  Compression • By pressure from an improperly applied plaster  Trauma during accidents • By fractures of the neck of the fibula  Ischemia • By compression ischaemia resulting from crossing the legs or adopting an unusual posture, such as squatting
- 8.  Cutaneous sensation is impaired over the lateral aspect of the lower leg and ankle and dorsum of the foot.  Reduced dorsiflexion and eversion of the foot and of toe extension • The patients will compensate by having a steppage gait.  N.B Inversion and plantar flexion are normal.
- 9. ď‚ž Progressive weakness of the peronei and tibialis anterior muscles which result in foot drop. ď‚ž The peroneus longus , tibialis anterior and the extensor digitorum wastes. ď‚ž N.B The paresis results in ankle weakness and predispose to ankle sprains
- 10. ď‚ž Deep peroneal nerve is rarely injured in the region of the ankle ď‚ž Usually injury is due to a tight-fitting rim or strap from a shoe. ď‚ž Pain in the region with minimal weakness and sensory disturbance involving only the web space between digits 1 and 2. ď‚ž Physical exam reveals minimal abnormalities. ď‚ž Nerve conduction studies demonstrate a prolonged distal motor latency.
- 11.  Assistive and adaptive devices and equipment. • Canes, crutches, or walkers may be used to help prevent falling, normalize gait patterns, or unload a painful weight-bearing limb.  Electrical Stimulation. • Transcutaneous electrical nerve stimulation (TENS) for the reduction or obliteration of pain.
- 12.  Positioning. • Correct positioning of limb  Protective Devices and Equipment eg splints, orthoses  Cryotherapy, massage
- 13. Sunderland S, Nerves and nerve injuries, 2nd edition, 1978, pages 974- 977  Mendell R et al, Diagnosis and management of peripheral nerve disorders, 2001, pages 621 – 625  Apley, System of orthopaedics and fractures, 5th edition, 1978, page 126  M. F. REINDERS, J. H. B. GEERTZEN and J. S. RIETMAN, Prosthetics and Orthotics International, 1996, 20, 197-198 
- 14. THANK YOU