Congenital Syphillis, Reccurent Apthae, Behcets and Reiter's Syndrome..
ŌĆóDownload as PPTX, PDFŌĆó
10 likesŌĆó4,320 views

Congenital syphilis occurs when a child is born to a mother with secondary syphilis. If a pregnant mother with syphilis is treated, especially before 16 weeks of pregnancy, it can effectively prevent congenital syphilis in the unborn child. Congenital syphilis can result in stillbirth, symptoms in the newborn like bone and teeth abnormalities, or a normal child. Recurrent aphthous stomatitis, or canker sores, are small ulcers that repeatedly form in the mouth and are thought to have multiple contributing factors including genetics, immunity, nutrition, trauma, and systemic disease. Beh├¦et's syndrome is characterized by recurrent oral and genital ulcers along with





































Congenital Syphillis, Reccurent Apthae, Behcets and Reiter's Syndrome..
- 3. ŌĆó Congenital syphilis is syphilis present in utero and at birth, and occurs when a child is born to a mother with secondary syphilis ŌĆó If a pregnant mother is identified as being infected with syphilis, treatment can effectively prevent congenital syphilis from developing in the unborn child, especially if she is treated before the sixteenth week of pregnancy ŌĆó Result in Still birth / congenital syphilis / normal child
- 4. ŌĆó Frontal bossing and short maxilla
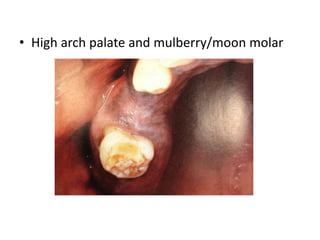
- 5. ŌĆó High arch palate and mulberry/moon molar
- 6. ŌĆó Saddle nose HigoumenakiŌĆÖs Sign
- 7. ŌĆó Rhagades Shaber shin
- 9. Treatment ŌĆó A woman in the secondary stage of syphilis decreases her child's risk of developing congenital syphilis by 98% if she receives treatment before the last month of pregnancy. ŌĆó An affected child can be treated using antibiotics much like an adult; however, any developmental symptoms are likely to be permanent
- 10. Recurrent Aphthous stomatitis ŌĆó also termed canker sores, recurrent aphthous stomatitis, RAS, recurring oral aphthae and recurrent aphthous ulceration ŌĆó repeated formation of ulcers in the mouth
- 11. Etiology ŌĆó The cause is not entirely clear, but is thought to be multifactorial ŌĆó Multiple research studies have attempted to identify a causative organism ŌĆó Genetic History ŌĆó Immunology ŌĆó Iron, Vitamin B, Folic Acid deficiency
- 12. Precipitating Factors ŌĆó Trauma ŌĆó Endocrine Factors ŌĆó Psychic Factors ŌĆó Allergic Factors ŌĆó Systemic Disease
- 13. Classification ŌĆó Recurrent Aphthous minor ŌĆó Recurrent Aphthous major ŌĆó Recurrent Herpetiform ulceration ŌĆó Associated with BehcetŌĆÖs syndrome
- 14. Clinical Features , Mikulicz ulcers ŌĆó They occur mainly in persons 10-40 years of age. ŌĆó They often cause pain and inability to eat . ŌĆó They are small round or ovoid ulcers 2-4 mm in diameter ŌĆó Ulcer floor that is yellowish but assumes a gray hue. ŌĆó Surrounded by an erythematous halo and some edema. ŌĆó They are found mainly on the nonkeratinized mobile mucosa. ŌĆó They occur in groups of only a few ulcers (ie, 1-6) at a time. ŌĆó They heal in 7-10 days. ŌĆó They leave little or no evidence of scarring.
- 16. Sutton ulcers ŌĆó They are larger, of longer duration, of more frequent recurrence, and often more painful. ŌĆó They are round or ovoid like MiAUs but are larger ŌĆó They reach a large size, usually about 1 cm or more ŌĆó They are found on any area of the oral mucosa ŌĆó They occur in groups of only a few ulcers (ie, 1-6) ŌĆó They heal slowly over 10-40 days. ŌĆó They recur extremely frequently. ŌĆó They may heal with scarring.
- 18. Herpetiform ulceration (HU) ŌĆó They are found in a slightly older age group, in females ŌĆó They begins with vesiculation that passes rapidly into multiple, minute, pinhead-sized, discrete ulcers. ŌĆó They involve any oral site, including the keratinized mucosa, increase in size, and coalesce to leave large round ragged ulcers. ŌĆó They heal in 10 days or longer. ŌĆó They are often extremely painful. ŌĆó They recur so frequently that ulceration may be virtually continuous.
- 20. Histologic Features... ŌĆó Ulceration ŌĆó Fibrinopurulent membrane ŌĆó Micro organism ŌĆó Granulation tissue ŌĆó Inflammation ŌĆó Endothelial cells ŌĆó Fibrosis
- 23. Treatment Modalities ŌĆó Antibiotics ŌĆó Antiseptics ŌĆó Diet Suppliment ŌĆó Symptomatic Treatment
- 24. Beh├¦et's syndrome ŌĆó Turkish dermatologist Hulusi Beh├¦et, 1937 ŌĆó a syndrome of recurrent aphthous ulcers, genital ulcerations, and uveitis leading to blindness. ŌĆó Etiology is proposed to be an infectious trigger, with inflammatory mediators and immune deregulation ŌĆó HLA B 51 ŌĆó Environmental Factors ŌĆó Infections
- 25. ŌĆó In 1990, the International Study Group (ISG) for Beh├¦et's Disease clarified criteria for the diagnosis of Beh├¦et disease ŌĆó Recurrent painful genital ulcers that heal with scarring ŌĆó Ophthalmic lesions, including anterior or posterior uveitis, hypopyon, or retinal vasculitis ŌĆó Skin lesions, including erythema nodosumŌĆōlike lesions, pseudofolliculitis, or papulopustular or acneiform lesions
- 27. Oral Lesions ŌĆó Painful oral lesions ŌĆó (aphthous or herpetiform) ŌĆó high recurrence rate ŌĆó multiple lesions or crops ŌĆó commonly found in ŌĆó keratinized areas
- 28. Skin lesions ŌĆó lesions often occur in the genital region of both sexes ŌĆó In males, scrotal, penile shaft. ŌĆó In females, the labial area, vagina and on the perineum ŌĆó Acneiform papulopustular lesions
- 29. Ocular Lesions ŌĆó anterior or posterior uveitis, hypopyon ŌĆó Symptoms commonly include blurred vision, periorbital pain, photophobia, and excessive lacrimation. ŌĆó Highly recurrent posterior uveitis can lead to blindness.
- 30. Lab Findings ŌĆó Hypergammaglobulinemia ŌĆó Leukocytosis with eosinophilia ŌĆó CRP, C9, C3 and C4 may be elevated
- 31. Treatment ŌĆó No specific treatment ŌĆó May spontaneously resolve or lead to death
- 32. ReiterŌĆÖs Syndrome ŌĆó characterized by a triad of balanitis, urethritis, and conjunctivitis, and by lesions of the skin and mucosal surfaces. ŌĆó Infectious origin ?? ŌĆó Mimics Gonorrhea ŌĆó Considered to be an immunodysregulated condition ŌĆó HLA B27
- 33. ŌĆó Urethritis is a common condition of Reiter's. This involves inflammation of the urethra ŌĆó Arthritis - experience swelling and tenderness ŌĆó conjunctivitis may develop. ŌĆó Skin lesions appear as small, painless sores on the head of the penis, roof of the mouth or tongue.
- 36. Treatment ŌĆó May undergo spontaneous remission ŌĆó Can be treated by antibiotics and corticosteroids...
- 41. Thank you...