CSC Form 211 - Medical Certificate.doc
ŌĆóDownload as DOC, PDFŌĆó
1 likeŌĆó1,398 views

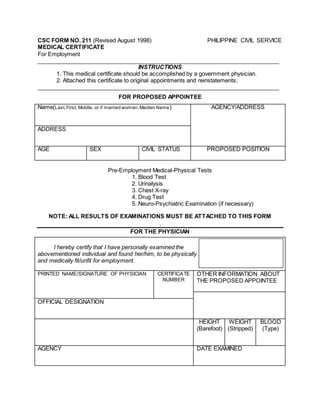
This medical certificate form is to be completed by a government physician for individuals being considered for employment or reinstatement. It requires basic personal information about the applicant as well as the results of various medical and physical tests, including blood tests, urinalysis, chest x-rays, and drug tests. The examining physician must then certify whether the applicant is physically and medically fit or unfit for the proposed position.
CSC Form 211 - Medical Certificate.doc
- 1. CSC FORM NO. 211 (Revised August 1998) PHILIPPINE CIVIL SERVICE MEDICAL CERTIFICATE For Employment ____________________________________________________________________________ INSTRUCTIONS 1. This medical certificate should be accomplished by a government physician. 2. Attached this certificate to original appointments and reinstatements. ____________________________________________________________________________ FOR PROPOSED APPOINTEE Name(Last,First, Middle, or if married woman,Maiden Name) AGENCY/ADDRESS ADDRESS AGE SEX CIVIL STATUS PROPOSED POSITION Pre-Employment Medical-Physical Tests 1. Blood Test 2. Urinalysis 3. Chest X-ray 4. Drug Test 5. Neuro-Psychiatric Examination (if necessary) NOTE: ALL RESULTS OF EXAMINATIONS MUST BE ATTACHED TO THIS FORM . FOR THE PHYSICIAN I hereby certify that I have personally examined the abovementioned individual and found her/him, to be physically and medically fit/unfit for employment. PRINTED NAME/SIGNATURE OF PHYSICIAN CERTIFICATE NUMBER OTHER INFORMATION ABOUT THE PROPOSED APPOINTEE OFFICIAL DESIGNATION HEIGHT (Barefoot) WEIGHT (Stripped) BLOOD (Type) AGENCY DATE EXAMINED