































More Related Content
What's hot (20)
Similar to Dialysis (20)

















Recently uploaded (20)




















Dialysis
- 1. DIALYSIS
- 2. Introduction Dialysis refers to diffusion of solid molecules through semipermeable membrane passing from higher concentration to lower concentration. The main purpose is to : ï§ Maintain fluid , electrolyte and acid base balance. ï§ To remove endogenous and exogenous toxins. It is substitute for some kidney excretory function but does not replace the kidneys endocrine function.
- 4. Haemodialysis ï§ Hemo = blood , dialysis = seprate ï§ It is the process of cleaning the blood of accumulated waste product. ï§ It is used for the patient who is acutely ill and and require short term dialysis (days to week ) and for the patients with advanced CKD and ESRD who required longterm or permanent treatment. It prevent death but donât cure disease. ï§ 3 times a week with an average 3-4 hours in outpatient settings.
- 5. Indication ï§ Clinical ïFluid overloads not responding to diuretics . ïUremic convulsion. ïPersistent dyspnea , vomiting and restlessness. ïSigns of pericarditis , pericardial effusion and ï pericardial frictional rub.
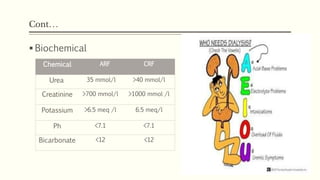
- 6. ContâĶ ï§ Biochemical Chemical ARF CRF Urea 35 mmol/l >40 mmol/l Creatinine >700 mmol/l >1000 mmol /l Potassium >6.5 meq /l 6.5 meq/l Ph <7.1 <7.1 Bicarbonate <12 <12
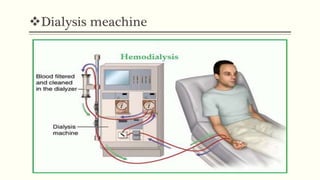
- 7. Requirements of hemodialysis ï§ Access to patient circulation . ï§ Dialysis machine . ï§ Dialyzer . ï§ Appropriate dialysate bath .
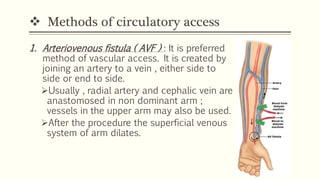
- 8. ïķ Methods of circulatory access 1. Arteriovenous fistula ( AVF ) : It is preferred method of vascular access. It is created by joining an artery to a vein , either side to side or end to side. ïUsually , radial artery and cephalic vein are anastomosed in non dominant arm ; vessels in the upper arm may also be used. ïAfter the procedure the superficial venous system of arm dilates.
- 9. Circulatory access contâĶ ïBy the means of 2 large bore needles inserted into the dilated venous system, blood may be obtained and passed thrugh the dialyzer. ïThe arterial end is used for arterial flow and the distal end is used for reinfusion of dialysed blood. ïHealing of AVF requires at least 6 to 8 weeks ; the centre vain is used for interim.
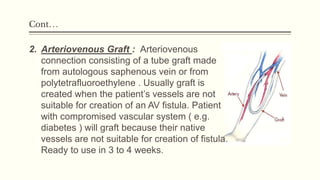
- 10. ContâĶ 2. Arteriovenous Graft : Arteriovenous connection consisting of a tube graft made from autologous saphenous vein or from polytetrafluoroethylene . Usually graft is created when the patientâs vessels are not suitable for creation of an AV fistula. Patient with compromised vascular system ( e.g. diabetes ) will graft because their native vessels are not suitable for creation of fistula. Ready to use in 3 to 4 weeks.
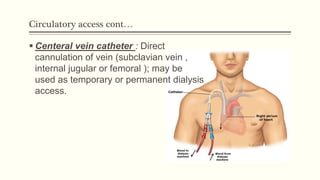
- 12. Circulatory access contâĶ ï§ Centeral vein catheter : Direct cannulation of vein (subclavian vein , internal jugular or femoral ); may be used as temporary or permanent dialysis access.
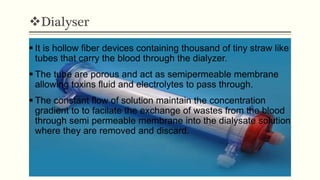
- 14. ïķDialyser ï§ It is hollow fiber devices containing thousand of tiny straw like tubes that carry the blood through the dialyzer. ï§ The tube are porous and act as semipermeable membrane allowing toxins fluid and electrolytes to pass through. ï§ The constant flow of solution maintain the concentration gradient to to facilate the exchange of wastes from the blood through semi permeable membrane into the dialysate solution where they are removed and discard.
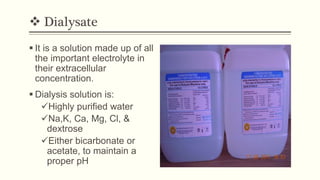
- 15. ïķ Dialysate ï§ It is a solution made up of all the important electrolyte in their extracellular concentration. ï§ Dialysis solution is: ïžHighly purified water ïžNa,K, Ca, Mg, Cl, & dextrose ïžEither bicarbonate or acetate, to maintain a proper pH
- 16. Physiological principles 1. Diffusion : The toxins and wastes in blood are removed by diffusion i.e they move from an area of higher concentration in blood to an area of lower concentration in the dialysate. 2. Osmosis : Excess water I removed from blood by osmosis , in which water move from an area of lower concentration potential to an area of high concentration potential. 3. Ultrafiltration : Created by increased pressure in the blood compartment or a decreased pressure in the dialysate compartment. In this water moves under high pressure to an area of low pressure.
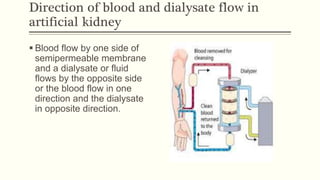
- 17. Direction of blood and dialysate flow in artificial kidney ï§ Blood flow by one side of semipermeable membrane and a dialysate or fluid flows by the opposite side or the blood flow in one direction and the dialysate in opposite direction.
- 18. Complications ï Acute Complications 1. Hypotension 2. Muscle cramp 3. Disequilibrium syndrome 4. Pruritus 5. Hypoglycemia 6. Hypokalemia 7. Dysrhythmia 8. Air embolus 9. Hemolysis
- 19. ContâĶ 1. Arterial disease 2. Hypertension 3. Anaemis 4. Osteodystrophy 5. Acquired renal cysts. 6. Malnutrition 8. Dialysis dementia 9. Respiratory problems 10.Endocraniopathies ï Chronic Complications
- 20. Care of blood access fistula or graft 1. Proper exercise by squeezing of hand . 2. Avoid heavy lifting . 3. Avoid pressure while sleeping . 4. Avoid any pricks . 5. Avoid taking BP on access hand. 6. Keep access clean all time, do not use any cream or lotions on the vascular site . 7. Avoid wearing jewellery and tight clothes .
- 21. ContâĶ 8. Listen for bruit at the site by placing the diaphragm of stethoscope gently on the site . 9. Check the functioning of vascular access several times a day by palpating the site for a thrill , which is buzzing or pulsing feeling that indicates good blood flow through the access site . 10.Assess the vascular site for any signs of infection such as redness , warmth , tenderness ,open sores and swelling .
- 23. Before dialysis 1. Explanation about the procedure /duration ,expected outcomes and possible complications . 2. Informed consent . 3. Collect all the investigations report . 4. Check vital signs :BP for hypo and hypertension; temperature for sepsis; respiration for fluid overload. 5. Weight: Determines amount of fluid to be removed during dialysis and patientâs clinical conditioning before starting . 6. Check efficiency of AV fistula .
- 24. ContâĶ 7. Review Medications : Hold drugs that pass through the dialysis membrane, such as piperacillin, folic acid, and other water-soluble vitamins. Hold antihypertensive drugs, especially if systolic pressure is below 100, per physician order . 8. Preparation of dialyzer âarterial venous tubing 9. Preparation of dialysis sets/area . 10.Setting of emergency cart . 11.Preparation of procedure area . 12.Start dialysis .
- 25. During dialysis 1. Monitor vital signs in every 15 minutes . 2. Provide comfortable position , diversional activities to promote comfort and help to pass time . 3. Assess for dialysis disequilibrium syndrome , with headache , nausea and vomiting , altered LOC , and hypertension .Rapid change in the BUN and electrolytes level lead to cerebral edema and increased ICP .
- 26. ContâĶ 4. Assess for the other responses to dialysis such as dehydration , nausea , vomiting , muscle cramps or seizure activity . 5. If a transfusion is given during dialysis , monitor for the possible transfusion reaction . 6. Assess for bleeding at the access site or elsewhere. Heparinization during dialysis increases the risk for bleeding.
- 27. After dialysis 1. Positioning of patient as comfortable . 2. Monitor vital signs and status of patient . 3. Carefully removing of arterial and venous tubing and apply effective pressure on that area to prevent bleeding . 4. Record the outcome . 5. Inform patient and visitors for next date of dialysis . 6. Explain about the home care including fistula care .