Distal End Radius Fractures - Colles, Smiths & Bartons
Download as PPTX, PDF95 likes27,072 views
ORTHOPEDICS Definition, Mechanism, Clinal features, Diagnosis and treatment of Colles, Smiths and Bartons Fracture in Distal end Radius.
1 of 27
Downloaded 522 times














Recommended
monteggia fracture
monteggia fractureGaurav Mehta
Ěý
This document discusses Monteggia fractures, which involve a fracture of the ulna bone in the forearm combined with a dislocation of the radial head. It begins with a historical description of the injury and provides details on epidemiology and classifications. Bado's classification system from 1958 divides Monteggia fractures into four main types based on the direction of radial head dislocation and location of the ulna fracture. The document discusses mechanisms of injury, clinical evaluation, radiographic assessment, non-operative and operative management approaches, potential complications, and emphasizes the importance of anatomic reduction and stabilization of both the ulna fracture and radial head dislocation.Shaft of humerus fracture
Shaft of humerus fractureBipulBorthakur
Ěý
1) Fractures of the humeral shaft can result from a fall on an outstretched hand or direct blow to the arm.
2) Treatment involves either hanging casts or surgery depending on the severity of the fracture and any complications.
3) Complications can include injury to the radial nerve and non-union of the bone fragments, so careful assessment of nerve function is important both before and after treatment.InterTrochanteric Fractures
InterTrochanteric FracturesKevin Ambadan
Ěý
An intertrochanteric fracture occurs between the greater and lesser trochanters of the femur. It commonly results from a fall in elderly osteoporotic patients. While internal fixation is usually required, sliding hip screws are the most widely used implant due to their ability to stabilize both stable and unstable fracture patterns. Complications can include malunion, cut out of fixation screws, and failure of the implant.smith fractures
smith fracturesAlhassan Alsalem
Ěý
Smith fractures are fractures of the distal radius where the distal fragment is displaced anteriorly, opposite to a Colles' fracture. They account for less than 3% of radius fractures and occur most commonly in young males and elderly females. Smith fractures can be extra-articular, intra-articular, or a fracture-dislocation. Patients present with wrist injury and a 'garden spade' deformity rather than the 'dinner fork' deformity of a Colles' fracture. X-rays show the distal fragment displaced anteriorly. Treatment involves closed reduction, casting, and possible fixation for unstable fractures.Galeazzi fracture dislocation
Galeazzi fracture dislocationrashree-singh
Ěý
Galeazzi fracture-dislocation is a fracture of the distal or middle third of the radius shaft combined with dislocation of the distal radioulnar joint. It most often occurs in males due to indirect trauma from a fall on an outstretched hand with rotation. Radiographs show the radial fracture and dislocation of the distal radioulnar joint. Treatment involves open reduction and internal fixation of the radial fracture with a plate while restoring length and stability of the distal radioulnar joint. The forearm is then immobilized in supination for 4-6 weeks to heal.Cubitus varus deformity
Cubitus varus deformityramachandra reddy
Ěý
Cubitus varus, or gunstock deformity, is caused by malunion of supracondylar fractures and results in the forearm being deviated inward at the elbow with loss of the carrying angle. It is a triplanar deformity involving varus, hyperextension, and internal rotation. Treatment options include observation for young children, hemiepiphysiodesis to alter growth, and corrective osteotomy. The lateral closing wedge osteotomy is commonly used to safely correct the varus deformity through removal of a lateral wedge. Other techniques include medial opening wedge, oblique, dome, and step-cut osteotomies. Postoperative management focuses on immobilizing the arm in extensionShoulder dislocation
Shoulder dislocationSCGH ED CME
Ěý
Shoulder dislocations have been documented as far back as ancient Egypt. The most common type is anterior dislocation, which accounts for 60% of cases. Reduction techniques described include external rotation, scapular manipulation, Milch, Stimson, traction-countertraction, and Spaso. Post-reduction, most patients are immobilized for 3 weeks if under 30 or begin mobilization after 1 week if over 30. Recurrent dislocation is a major complication, seen in 50-90% of patients under 20.Supracondylar Fractures
Supracondylar FracturesPulasthi Kanchana
Ěý
An Introduction, Biomechanics, Radiological Diagnosis, Management of Suracondylar Fractures of Children.supracondylar fracture humerus in children
supracondylar fracture humerus in childrenHardik Pawar
Ěý
Supracondylar fractures of the humerus are the most common elbow injuries in children, making up approximately 60% of cases. They typically occur as a result of a fall onto an outstretched hand in children aged 5-7 years old. Radiographs are used to classify fractures as non-displaced (Type I), displaced with an intact posterior cortex (Type II), or completely displaced (Type III). Posteromedial displacement is more common than posterolateral. Physical examination focuses on evaluating neurovascular status and detecting any S-shaped deformity, with nerve injuries occurring in up to 16% of cases.Elbow dislocations
Elbow dislocationsAjith John
Ěý
1. Elbow dislocations are most commonly caused by falls onto an outstretched hand and involve the disruption of the lateral and medial collateral ligaments and elbow capsule.
2. Simple elbow dislocations without fractures are typically treated non-operatively with closed manipulation and immobilization for less than 3 weeks to avoid stiffness.
3. Operative treatment is considered if closed reduction cannot be maintained or for recurrent dislocations and involves repair of the lateral collateral ligaments through bone tunnels or anchors. Fracture shaft of femur
Fracture shaft of femurPrakat Aryal
Ěý
The document discusses fracture of the shaft of the femur. It begins by describing the anatomy of the femur bone and its role in weight bearing. It then discusses the clinical presentation, mechanisms, imaging, and management of femoral shaft fractures. Femoral shaft fractures are typically caused by high-energy trauma and present with thigh pain and swelling. Imaging includes x-rays to diagnose the fracture. Management involves resuscitation, splinting, and either non-operative treatment with traction or operative treatment with intramedullary nailing or plating depending on the fracture pattern and patient factors.Ankle fractures
Ankle fracturesDr.Anshu Sharma
Ěý
Ankle fractures are common injuries that require careful evaluation to identify bony and soft tissue damage. The ankle is a complex hinge joint supported by ligaments and the tibia, fibula, talus, and deltoid ligament. Classification systems like Lauge-Hansen and Weber are used to characterize fracture patterns and guide management, which may involve closed treatment for stable injuries or surgery to restore ankle anatomy and stability for unstable fractures. Radiographs are important for diagnosis but CT or MRI may be needed to fully evaluate injury extent.Radial nerve palsy
Radial nerve palsymanoj das
Ěý
The document provides information about the radial nerve including its anatomy, course, branches and clinical presentations of radial nerve palsies. It discusses the radial nerve's origin from the brachial plexus and branches in the arm and forearm. Common causes of radial nerve palsy include fractures and entrapment in the radial tunnel. Clinical features, investigations, treatment including splinting and tendon transfers, and postoperative management are outlined. Surgical techniques for nerve repair and reconstructive procedures are also described.Supracondylar fracture of humerus
Supracondylar fracture of humerusBipulBorthakur
Ěý
This document discusses supracondylar fractures of the humerus, which occur most commonly in children ages 5-10 years old. It describes the anatomy of the elbow joint and mechanisms of injury for supracondylar fractures. The Gartland classification system grades the fractures from non-displaced to severely displaced. Treatment depends on the fracture type, with non-displaced fractures treated conservatively and displaced fractures requiring closed or open reduction with pin fixation. Complications can include vascular injury, nerve injury, compartment syndrome, malunion, and elbow stiffness.Colles' fracture 
Colles' fracture akond1986
Ěý
Mahashin akond presented on Colles' fracture, which is a break in the distal part of the radius bone 2.5cm above the articular surface. Colles' fractures most commonly occur in young adults and those over 40 years old from falls or direct blows. Treatment involves reduction, immobilization with a plaster cast or surgery, followed by physiotherapy to regain range of motion, strength, and function. Complications can include malunion, tendon rupture, osteoporosis, and delayed healing, though most fractures heal within 6-8 weeks with proper treatment and rehabilitation.Tuberculosis of hip
Tuberculosis of hipHardik Pawar
Ěý
Tuberculosis of the hip is caused by Mycobacterium tuberculosis infection. It typically affects people aged 20-30 years old. The infection spreads hematogenously from a primary focus and causes destruction of bone and joints over several years. Clinical features include limping, decreased range of motion, and deformities in advanced cases. Imaging shows osteopenia, joint space narrowing, and bone erosion. Treatment involves chemotherapy for at least 6-9 months along with local measures like joint aspiration and traction. Surgery may be needed for debridement, arthrodesis, or arthroplasty in advanced cases.Colles fracture
Colles fractureDr.Monica Dhanani
Ěý
Colles' fracture is a fracture of the distal radius near the wrist. It often results in dorsal displacement of the distal fragment and occurs most commonly in women over 40 from falls on an outstretched hand. Clinical features include pain, swelling, and the classic "dinner fork deformity". Treatment depends on the degree of displacement, with undisplaced fractures treated conservatively in a cast and displaced fractures requiring manipulative closed reduction and casting or open surgical fixation with plates. Complications can include joint stiffness, malunion, subluxation, and nerve damage if not properly treated.Congenital talipes equinovarus (club foot/ctev) ppt by Dr Pratik
Congenital talipes equinovarus (club foot/ctev) ppt by Dr PratikDr. Pratik Agarwal
Ěý
ctev (club foot) with its aetiology, pathological anatomy, classification, non surgical and surgical treatmentNon Union
Non UnionAbdullah Mamun
Ěý
This presentation was prepared for a AOSEC course in Chittagong, Bangladesh. This course was organized by AO Foundation.perthes disease 
perthes disease BipulBorthakur
Ěý
This document provides an overview of Legg Calve Perthes disease, including its definition, demographics, risk factors, pathogenesis, clinical features, investigations, classifications, management, and surgical procedures. Some key points:
- It is avascular necrosis of the femoral head in children, most common in ages 4-8 years. Positive family history and low birth weight are risk factors.
- Clinical features include hip/thigh pain aggravated by movement. Imaging shows stages from avascular necrosis to fragmentation to regeneration/healing.
- Conservative management includes bracing for young/mild cases. Surgical containment is used for more severe/older cases to encourage spherical remodeling.
- ProceduresNeck of femur fractures
Neck of femur fracturesBADAL BALOCH
Ěý
This document discusses neck of femur fractures (NOF), also known as hip fractures. It covers the epidemiology, risk factors, anatomy, classification, diagnosis, and treatment of NOF fractures. NOF fractures typically occur in elderly patients from low-energy falls and are associated with osteoporosis, while in younger patients they usually result from high-energy injuries. Treatment depends on factors like the patient's age, health, and fracture classification, and may involve closed or open reduction, fixation with screws or nails, or arthroplasty. Complications can include nonunion, osteonecrosis, fixation failure, dislocation, and increased mortality risk especially in older or less healthy patients.AVASCULAR NECROSIS OF HIP (AVN HIP)
AVASCULAR NECROSIS OF HIP (AVN HIP)Dr.A.Mohan krishna
Ěý
This is a short presentation on avascular necrosis of femoral head. This presentation gives brief description of causes of AVN, investigations and modes of treatment options available.
AVN TREATMENT IN HYDERABAD
Core decompression for AVN
Stem cell treatment for AVN
Surgery for AVN
Avascular necrosis treatment options
Hip replacement in hyderabad
Hip specialist in hyderabad
Hip surgery in hyderabad
Total hip replacement in hyderabad
cemented hip replacement
uncemented hip replacement in hyderabad
ceramic hip replacement
delta motion hip
ceramic on ceramic hip replacement
metal on poly hip replacement
affordable hip replacement in hyderabad
Fractures of distal end radius
Fractures of distal end radiusMahak Jain
Ěý
This document provides information on fractures of the distal end of the radius bone. It discusses the history, incidence, anatomy, classification, diagnosis, and treatment options for these fractures. Distal radius fractures most commonly result from falls on an outstretched hand and occur in three main age groups. Treatment depends on factors like fracture pattern and stability, and may involve closed reduction with casting or surgical options like percutaneous pinning, plating, or external fixation. The goals of treatment are to restore function, alignment, and stability while avoiding complications.Humeral shaft fractures
Humeral shaft fracturesSupun Dhanasekara
Ěý
Humeral shaft fractures are fractures of the upper arm bone between the shoulder and elbow. They make up 3-5% of all fractures. Most heal with conservative care like splinting or bracing, though some require surgery. Risk of complications is higher with more displaced or open fractures. Treatment depends on fracture type and stability, with options including splinting, bracing, plating, nailing, or external fixation. Potential complications include nonunion, malunion, nerve injuries, and joint stiffness.Forearm fractures
Forearm fracturesMohamed Fazly
Ěý
The document discusses the anatomy and classification of forearm fractures. It describes the radius and ulna bones of the forearm and their articulations. Forearm fractures can be classified as proximal, middle, or distal, and can affect one or both bones. Common types include radial shaft fractures, Galeazzi fractures, and Monteggia's fractures. Assessment involves neurovascular and range of motion exams. Treatment depends on the fracture type but may include immobilization, closed reduction, open reduction and internal fixation, or external fixation.Patella fracture
Patella fractureDr. Vitthalrao Vikhe Patil Foundation's College of Physiotherapy, Ahmednagar
Ěý
This document summarizes information about fractures of the patella. It describes the anatomy of the patella and mechanisms of injury, which can include direct trauma from a fall or indirect trauma from forceful quadriceps contraction. Clinical evaluation involves examining for pain, swelling, abrasions, and limited knee movement. Fractures are classified as undisplaced or displaced. Investigations may include x-rays, CT scans, bone scans, and MRIs. Treatment depends on the type of fracture, and may involve casting, tension band wiring, or patellectomy. Complications can include non-union, avascular necrosis, osteoarthritis, or knee stiffness.Clinical Examination of Hip
Clinical Examination of HipVivek Mathew Philip
Ěý
The document provides information on clinical examination of the hip joint. It begins with anatomy of the hip joint and associated muscles and ligaments. It then discusses elements of history taking including pain characteristics. The physical examination section covers inspection of gait, limb posture and length, palpation of bony landmarks and muscles, range of motion testing, and special tests like Trendelenburg test. Measurements of limb length discrepancies both apparent and true are also described.Perthes ’ disease
Perthes ’ diseaseMannan Ahmed
Ěý
This document provides information about Perthes' disease, including:
- It is characterized by avascular necrosis of the femoral head in children.
- Risk factors include being male and between ages 5-10 years old.
- Imaging studies like x-rays are used to diagnose and monitor the stages of avascular necrosis, fragmentation, ossification, and remodeling.
- Differential diagnosis depends on whether the condition is unilateral or bilateral.
- Treatment aims to prevent deformity through nonsurgical or surgical methods depending on the severity.Distal end radius, monteggia and galleazi fractures.
Distal end radius, monteggia and galleazi fractures.Dialla Sandouka
Ěý
a simple approach to ditsal end radius, monteggia and galleazi fractures. made by a 5th year medical student at NNU
More Related Content
What's hot (20)
supracondylar fracture humerus in children
supracondylar fracture humerus in childrenHardik Pawar
Ěý
Supracondylar fractures of the humerus are the most common elbow injuries in children, making up approximately 60% of cases. They typically occur as a result of a fall onto an outstretched hand in children aged 5-7 years old. Radiographs are used to classify fractures as non-displaced (Type I), displaced with an intact posterior cortex (Type II), or completely displaced (Type III). Posteromedial displacement is more common than posterolateral. Physical examination focuses on evaluating neurovascular status and detecting any S-shaped deformity, with nerve injuries occurring in up to 16% of cases.Elbow dislocations
Elbow dislocationsAjith John
Ěý
1. Elbow dislocations are most commonly caused by falls onto an outstretched hand and involve the disruption of the lateral and medial collateral ligaments and elbow capsule.
2. Simple elbow dislocations without fractures are typically treated non-operatively with closed manipulation and immobilization for less than 3 weeks to avoid stiffness.
3. Operative treatment is considered if closed reduction cannot be maintained or for recurrent dislocations and involves repair of the lateral collateral ligaments through bone tunnels or anchors. Fracture shaft of femur
Fracture shaft of femurPrakat Aryal
Ěý
The document discusses fracture of the shaft of the femur. It begins by describing the anatomy of the femur bone and its role in weight bearing. It then discusses the clinical presentation, mechanisms, imaging, and management of femoral shaft fractures. Femoral shaft fractures are typically caused by high-energy trauma and present with thigh pain and swelling. Imaging includes x-rays to diagnose the fracture. Management involves resuscitation, splinting, and either non-operative treatment with traction or operative treatment with intramedullary nailing or plating depending on the fracture pattern and patient factors.Ankle fractures
Ankle fracturesDr.Anshu Sharma
Ěý
Ankle fractures are common injuries that require careful evaluation to identify bony and soft tissue damage. The ankle is a complex hinge joint supported by ligaments and the tibia, fibula, talus, and deltoid ligament. Classification systems like Lauge-Hansen and Weber are used to characterize fracture patterns and guide management, which may involve closed treatment for stable injuries or surgery to restore ankle anatomy and stability for unstable fractures. Radiographs are important for diagnosis but CT or MRI may be needed to fully evaluate injury extent.Radial nerve palsy
Radial nerve palsymanoj das
Ěý
The document provides information about the radial nerve including its anatomy, course, branches and clinical presentations of radial nerve palsies. It discusses the radial nerve's origin from the brachial plexus and branches in the arm and forearm. Common causes of radial nerve palsy include fractures and entrapment in the radial tunnel. Clinical features, investigations, treatment including splinting and tendon transfers, and postoperative management are outlined. Surgical techniques for nerve repair and reconstructive procedures are also described.Supracondylar fracture of humerus
Supracondylar fracture of humerusBipulBorthakur
Ěý
This document discusses supracondylar fractures of the humerus, which occur most commonly in children ages 5-10 years old. It describes the anatomy of the elbow joint and mechanisms of injury for supracondylar fractures. The Gartland classification system grades the fractures from non-displaced to severely displaced. Treatment depends on the fracture type, with non-displaced fractures treated conservatively and displaced fractures requiring closed or open reduction with pin fixation. Complications can include vascular injury, nerve injury, compartment syndrome, malunion, and elbow stiffness.Colles' fracture
Colles' fracture akond1986
Ěý
Mahashin akond presented on Colles' fracture, which is a break in the distal part of the radius bone 2.5cm above the articular surface. Colles' fractures most commonly occur in young adults and those over 40 years old from falls or direct blows. Treatment involves reduction, immobilization with a plaster cast or surgery, followed by physiotherapy to regain range of motion, strength, and function. Complications can include malunion, tendon rupture, osteoporosis, and delayed healing, though most fractures heal within 6-8 weeks with proper treatment and rehabilitation.Tuberculosis of hip
Tuberculosis of hipHardik Pawar
Ěý
Tuberculosis of the hip is caused by Mycobacterium tuberculosis infection. It typically affects people aged 20-30 years old. The infection spreads hematogenously from a primary focus and causes destruction of bone and joints over several years. Clinical features include limping, decreased range of motion, and deformities in advanced cases. Imaging shows osteopenia, joint space narrowing, and bone erosion. Treatment involves chemotherapy for at least 6-9 months along with local measures like joint aspiration and traction. Surgery may be needed for debridement, arthrodesis, or arthroplasty in advanced cases.Colles fracture
Colles fractureDr.Monica Dhanani
Ěý
Colles' fracture is a fracture of the distal radius near the wrist. It often results in dorsal displacement of the distal fragment and occurs most commonly in women over 40 from falls on an outstretched hand. Clinical features include pain, swelling, and the classic "dinner fork deformity". Treatment depends on the degree of displacement, with undisplaced fractures treated conservatively in a cast and displaced fractures requiring manipulative closed reduction and casting or open surgical fixation with plates. Complications can include joint stiffness, malunion, subluxation, and nerve damage if not properly treated.Congenital talipes equinovarus (club foot/ctev) ppt by Dr Pratik
Congenital talipes equinovarus (club foot/ctev) ppt by Dr PratikDr. Pratik Agarwal
Ěý
ctev (club foot) with its aetiology, pathological anatomy, classification, non surgical and surgical treatmentNon Union
Non UnionAbdullah Mamun
Ěý
This presentation was prepared for a AOSEC course in Chittagong, Bangladesh. This course was organized by AO Foundation.perthes disease
perthes disease BipulBorthakur
Ěý
This document provides an overview of Legg Calve Perthes disease, including its definition, demographics, risk factors, pathogenesis, clinical features, investigations, classifications, management, and surgical procedures. Some key points:
- It is avascular necrosis of the femoral head in children, most common in ages 4-8 years. Positive family history and low birth weight are risk factors.
- Clinical features include hip/thigh pain aggravated by movement. Imaging shows stages from avascular necrosis to fragmentation to regeneration/healing.
- Conservative management includes bracing for young/mild cases. Surgical containment is used for more severe/older cases to encourage spherical remodeling.
- ProceduresNeck of femur fractures
Neck of femur fracturesBADAL BALOCH
Ěý
This document discusses neck of femur fractures (NOF), also known as hip fractures. It covers the epidemiology, risk factors, anatomy, classification, diagnosis, and treatment of NOF fractures. NOF fractures typically occur in elderly patients from low-energy falls and are associated with osteoporosis, while in younger patients they usually result from high-energy injuries. Treatment depends on factors like the patient's age, health, and fracture classification, and may involve closed or open reduction, fixation with screws or nails, or arthroplasty. Complications can include nonunion, osteonecrosis, fixation failure, dislocation, and increased mortality risk especially in older or less healthy patients.AVASCULAR NECROSIS OF HIP (AVN HIP)
AVASCULAR NECROSIS OF HIP (AVN HIP)Dr.A.Mohan krishna
Ěý
This is a short presentation on avascular necrosis of femoral head. This presentation gives brief description of causes of AVN, investigations and modes of treatment options available.
AVN TREATMENT IN HYDERABAD
Core decompression for AVN
Stem cell treatment for AVN
Surgery for AVN
Avascular necrosis treatment options
Hip replacement in hyderabad
Hip specialist in hyderabad
Hip surgery in hyderabad
Total hip replacement in hyderabad
cemented hip replacement
uncemented hip replacement in hyderabad
ceramic hip replacement
delta motion hip
ceramic on ceramic hip replacement
metal on poly hip replacement
affordable hip replacement in hyderabad
Fractures of distal end radius
Fractures of distal end radiusMahak Jain
Ěý
This document provides information on fractures of the distal end of the radius bone. It discusses the history, incidence, anatomy, classification, diagnosis, and treatment options for these fractures. Distal radius fractures most commonly result from falls on an outstretched hand and occur in three main age groups. Treatment depends on factors like fracture pattern and stability, and may involve closed reduction with casting or surgical options like percutaneous pinning, plating, or external fixation. The goals of treatment are to restore function, alignment, and stability while avoiding complications.Humeral shaft fractures
Humeral shaft fracturesSupun Dhanasekara
Ěý
Humeral shaft fractures are fractures of the upper arm bone between the shoulder and elbow. They make up 3-5% of all fractures. Most heal with conservative care like splinting or bracing, though some require surgery. Risk of complications is higher with more displaced or open fractures. Treatment depends on fracture type and stability, with options including splinting, bracing, plating, nailing, or external fixation. Potential complications include nonunion, malunion, nerve injuries, and joint stiffness.Forearm fractures
Forearm fracturesMohamed Fazly
Ěý
The document discusses the anatomy and classification of forearm fractures. It describes the radius and ulna bones of the forearm and their articulations. Forearm fractures can be classified as proximal, middle, or distal, and can affect one or both bones. Common types include radial shaft fractures, Galeazzi fractures, and Monteggia's fractures. Assessment involves neurovascular and range of motion exams. Treatment depends on the fracture type but may include immobilization, closed reduction, open reduction and internal fixation, or external fixation.Patella fracture
Patella fractureDr. Vitthalrao Vikhe Patil Foundation's College of Physiotherapy, Ahmednagar
Ěý
This document summarizes information about fractures of the patella. It describes the anatomy of the patella and mechanisms of injury, which can include direct trauma from a fall or indirect trauma from forceful quadriceps contraction. Clinical evaluation involves examining for pain, swelling, abrasions, and limited knee movement. Fractures are classified as undisplaced or displaced. Investigations may include x-rays, CT scans, bone scans, and MRIs. Treatment depends on the type of fracture, and may involve casting, tension band wiring, or patellectomy. Complications can include non-union, avascular necrosis, osteoarthritis, or knee stiffness.Clinical Examination of Hip
Clinical Examination of HipVivek Mathew Philip
Ěý
The document provides information on clinical examination of the hip joint. It begins with anatomy of the hip joint and associated muscles and ligaments. It then discusses elements of history taking including pain characteristics. The physical examination section covers inspection of gait, limb posture and length, palpation of bony landmarks and muscles, range of motion testing, and special tests like Trendelenburg test. Measurements of limb length discrepancies both apparent and true are also described.Perthes ’ disease
Perthes ’ diseaseMannan Ahmed
Ěý
This document provides information about Perthes' disease, including:
- It is characterized by avascular necrosis of the femoral head in children.
- Risk factors include being male and between ages 5-10 years old.
- Imaging studies like x-rays are used to diagnose and monitor the stages of avascular necrosis, fragmentation, ossification, and remodeling.
- Differential diagnosis depends on whether the condition is unilateral or bilateral.
- Treatment aims to prevent deformity through nonsurgical or surgical methods depending on the severity.Similar to Distal End Radius Fractures - Colles, Smiths & Bartons (20)
Distal end radius, monteggia and galleazi fractures.
Distal end radius, monteggia and galleazi fractures.Dialla Sandouka
Ěý
a simple approach to ditsal end radius, monteggia and galleazi fractures. made by a 5th year medical student at NNUNamed fractures of forearm ,wrist &and hand
Named fractures of forearm ,wrist &and handJim Jacob Roy
Ěý
A presentation about the named fractures of forearm,wrist & hand - it will be useful for undergraduates learning orthopaedics .imaging in Appendicular and Pelvic Trauma.pptx
imaging in Appendicular and Pelvic Trauma.pptxhulkie8606
Ěý
Radiological imaging features of trauma in the setting of appendicular skeleton and the pelvic bones. detailed imaging and protocols for management. common INJURIES occuring around the ANKLE JOINT
common INJURIES occuring around the ANKLE JOINTraysdendanford
Ěý
this presentation discuses the most common injuries that occcur arround the ankle joint ant its managementElbow Injuries.pptx
Elbow Injuries.pptxesicOrtho1
Ěý
This document discusses various elbow injuries. It begins by describing elbow anatomy and development of the elbow bones in children. It then discusses common elbow fractures in children such as supracondylar fractures, lateral condyle fractures, and radial neck fractures. Treatment options for displaced and non-displaced fractures are provided. The document also discusses complications of fractures and injuries commonly seen in adults such as olecranon fractures, radial head fractures, and elbow dislocations. Surgical treatment techniques like tension band wiring and plating are described.Introduction to Upper limb trauma
Introduction to Upper limb traumaPrateek Goel
Ěý
1) The document discusses various types of upper limb trauma including fractures and dislocations of the shoulder, elbow, forearm, wrist and hand.
2) Signs and symptoms, mechanisms of injury, clinical evaluation including relevant tests and imaging, complications and treatment options are described for conditions like shoulder dislocation, humeral fractures, supracondylar humerus fractures, forearm fractures and wrist fractures.
3) Common fractures discussed include Colles fracture of distal radius, supracondylar humerus fractures in children, lateral condyle humerus fracture and Bennett's and Rolando fractures of the thumb.
4) Different types of splints used for immobilization like K wire splint,collesfracture-161020112314.pdf
collesfracture-161020112314.pdfmunirmemon40
Ěý
Colles' fracture is a fracture of the distal radius near the wrist. It often results in dorsal displacement of the distal fragment and occurs most commonly in women over 40 from falls on an outstretched hand. Clinical features include pain, swelling, and the classic "dinner fork deformity". Treatment depends on the degree of displacement, with undisplaced fractures treated conservatively in a cast and displaced fractures requiring manipulative closed reduction and casting or open surgical fixation with plates. Complications can include wrist stiffness, malunion, subluxation of the distal radio-ulnar joint, and tendon injuries.Upper limb fractures 
Upper limb fractures nooralsoub1
Ěý
The document summarizes common upper limb fractures including fractures of the elbow, forearm, and hand. It describes the mechanism, clinical presentation, treatment options, and potential complications for radial head fractures, Monteggia's fracture-dislocation, Galeazzi fracture-dislocation, Colles' fracture, Smith's fracture, scaphoid fracture, boxer's fracture, mallet finger, and avulsion of the flexor tendon. Treatment may involve closed or open reduction with immobilization in a cast or internal fixation depending on the fracture type and degree of displacement. Complications can include joint stiffness, nonunion, malunion, and nerve injuries.upper limb trauma.pptx
upper limb trauma.pptxrohanjohnjacob
Ěý
1. The document discusses various types of upper limb trauma including fractures of the clavicle, humerus, forearm, and distal radius as well as dislocations of the shoulder and elbow.
2. Key fracture classifications discussed include the Allman classification for clavicle fractures, Neer classification for proximal humerus fractures, and Bado's classification for Monteggia fractures.
3. Common mechanisms of injury involve falls onto an outstretched arm. Imaging workup involves radiographs to identify fracture patterns and displacements.Distal radius fractures
Distal radius fracturesDr Padma C Anand
Ěý
This document discusses distal radius fractures, which make up 20% of orthopaedic admissions. It describes the anatomy of the distal radius and classifications of fractures. Common types include Colles, Smith, Barton, and die punch fractures. Treatment depends on factors like patient age and fracture stability/displacement, and may involve closed or open reduction with pinning or plating to restore normal anatomy. Nonoperative treatment uses casting for stable fractures, while unstable fractures often require surgical fixation.Fracture of distal radius
Fracture of distal radiushanisahwarrior
Ěý
My seminar presentation slides. Please correct me if I've did something wrong in it. You can also leave any message thru my email, nurhanisahzainoren@gmail.comSpinal Fractures.pptx
Spinal Fractures.pptxkezias7
Ěý
Spinal fractures can occur in various locations and have different morphologies. Chalk stick fractures occur in fused spines like ankylosing spondylitis. Spinal compression fractures most often result from osteoporosis and cause vertebral height loss. Burst fractures involve disruption of the vertebral endplate and retropulsion of bone fragments into the spinal canal. Wedge fractures cause vertebral wedging from hyperextension injuries. Chance fractures extend through the vertebrae and posterior elements from high-energy flexion injuries.DISTAL END OF RADIUS FRACTURE AND DISLOCATION MANAGEMENT.pptx
DISTAL END OF RADIUS FRACTURE AND DISLOCATION MANAGEMENT.pptxpradeepreddyseelam1
Ěý
The document discusses the anatomy, classifications, and management of fractures of the distal radius. It begins with the anatomy of the distal radius and its articulations. It then covers several common classification systems for distal radius fractures, including the AO/ASIF classification and the Melone classification. The document discusses indications for closed versus open treatment, as well as techniques for closed and open reduction. Key points include maintaining length, tilt, and alignment during treatment. Surgical options like percutaneous pinning, external fixation, and various plating techniques are also summarized.Fractures around elbow lateral condyle and intercondylar fractures
Fractures around elbow lateral condyle and intercondylar fracturesSiddhartha Sinha
Ěý
Fractures around the elbow include lateral condyle fractures and intercondylar fractures. Lateral condyle fractures involve the lateral epicondyle and account for 17% of distal humeral fractures in children. They often result in less satisfactory outcomes than supracondylar fractures due to missed diagnoses and loss of motion. Intercondylar fractures involve a T or Y-shaped fracture line through the two humeral condyles and comminution is common. Both fracture types are typically treated operatively with open reduction and internal fixation to restore the joint surface and columns. Complications can include post-traumatic arthritis, failure of fixation, loss of motion, and neurologic injury. Fractures around elbow lateral condyle and intercondylar fractures
Fractures around elbow lateral condyle and intercondylar fracturesSiddhartha Sinha
Ěý
1) Lateral condyle fractures and intercondylar fractures of the elbow involve fractures around the lower end of the humerus.
2) Lateral condyle fractures, which account for 17% of distal humeral fractures in children, often require fixation to prevent nonunion. Intercondylar fractures in adults involve a T or Y-shaped fracture through the two humeral condyles.
3) Treatment depends on the type and severity of the fracture, ranging from casting for nondisplaced fractures to open reduction and internal fixation for displaced fractures to prevent long-term complications like nonunion and deformity.Ankle seminar
Ankle seminarArun Sivaram
Ěý
This document discusses ankle fractures, including their epidemiology, anatomy, classification systems, evaluation, and management. Some key points:
- Ankle fractures most often result from road traffic accidents or falls and twisting injuries. Left untreated, they can cause long-term pain, instability, and arthritis.
- The ankle joint is stabilized by bones, ligaments, tendons, and the fibrous capsule. Common fracture patterns include lateral malleolus, medial malleolus, and syndesmotic injuries.
- Classification systems include Lauge-Hansen (based on mechanism of injury), Weber (based on fibular fracture location), and OTA (describing bony patterns). Evaluation involves clinicalElbow FRACTURE
Elbow FRACTUREYadlapalli Anilkumar
Ěý
This document discusses various types of fractures of the distal humerus. It begins by describing distal humerus fractures in general, including common mechanisms of injury and clinical features. It then discusses specific fracture types - supracondylar, intercondylar, condylar, trochlear, and capitellar - providing details on classification systems, treatment options, and potential complications for each. Measurement techniques for radiographic evaluation and several classification systems used for distal humerus fractures are also summarized.Shoulder fractures around the shoulder 
Shoulder fractures around the shoulder bibincmc
Ěý
This document discusses fractures around the shoulder joint, including proximal humerus fractures, shoulder dislocations, scapular fractures, and clavicular fractures. It provides details on the anatomy, classifications, clinical presentations, imaging, and treatment options for each type of injury. Treatment may involve closed reduction, open reduction with various surgical techniques like plating or nailing depending on the fracture pattern and bone quality. Post-operative rehabilitation is important for optimal outcomes.upper limb trauma.pptx
upper limb trauma.pptxrohanjohnjacob
Ěý
1) Clavicle fractures are most commonly caused by falls onto the shoulder. Treatment is usually closed with immobilization, though surgery may be used for displaced or unstable fractures.
2) Proximal humerus fractures are also often caused by falls, and are evaluated clinically and radiographically. Treatment depends on fracture type and degree of displacement, ranging from immobilization to open reduction and internal fixation.
3) Shoulder dislocations, especially anterior dislocations, commonly cause Bankart lesions of the labrum and Hill-Sachs defects of the humeral head. Early surgical repair may be needed for recurrent instability.Recently uploaded (20)
legal Rights of individual, children and women.pptx
legal Rights of individual, children and women.pptxRishika Rawat
Ěý
A legal right is a claim or entitlement that is recognized and protected by the law. It can also refer to the power or privilege that the law grants to a person. Human rights include the right to life and liberty, freedom from slavery and torture, freedom of opinion and expression, the right to work and educationMultimodal Approaches to Clitoral Augmentation for FGM (PRP _ filler)"
Multimodal Approaches to Clitoral Augmentation for FGM (PRP _ filler)"Rehab Aboshama
Ěý
Multimodal Approaches to Clitoral Augmentation for FGM (PRP _ filler)"
Diabetic Ketoacidosis (DKA) & Its Management Protocol
Diabetic Ketoacidosis (DKA) & Its Management ProtocolDr Anik Roy Chowdhury
Ěý
Dr. Anik Roy Chowdhury
MBBS, BCS(Health), DA, MD (Resident)
Department of Anesthesiology, ICU & Pain Medicine
Shaheed Suhrawardy Medical College Hospital (ShSMCH)Renal Physiology - Regulation of GFR and RBF
Renal Physiology - Regulation of GFR and RBFMedicoseAcademics
Ěý
1. Explain the physiological control of glomerular filtration and renal blood flow
2. Describe the humoral and autoregulatory feedback mechanisms that mediate the autoregulation of renal plasma flow and glomerular filtration rate
Optimization in Pharmaceutical Formulations: Concepts, Methods & Applications
Optimization in Pharmaceutical Formulations: Concepts, Methods & ApplicationsKHUSHAL CHAVAN
Ěý
This presentation provides a comprehensive overview of optimization in pharmaceutical formulations. It explains the concept of optimization, different types of optimization problems (constrained and unconstrained), and the mathematical principles behind formulation development. Key topics include:
Methods for optimization (Sequential Simplex Method, Classical Mathematical Methods)
Statistical analysis in optimization (Mean, Standard Deviation, Regression, Hypothesis Testing)
Factorial Design & Quality by Design (QbD) for process improvement
Applications of optimization in drug formulation
This resource is beneficial for pharmaceutical scientists, R&D professionals, regulatory experts, and students looking to understand pharmaceutical process optimization and quality by design approaches.PresentaciĂł "Projecte Benestar". MWC 2025
PresentaciĂł "Projecte Benestar". MWC 2025Badalona Serveis Assistencials
Ěý
Presentació que va acompanyar la demostració prà ctica de metge d'Innovació José Ferrer sobre el projecte Benestar de BSA, nom d'IDIAP Pere Gol, el 5 de març de 2025 a l'estand de XarSMART al Mobible Word Congress. HUMAN SEXUALITY AND SEXUAL RESPONCE CYCLE
HUMAN SEXUALITY AND SEXUAL RESPONCE CYCLEdaminipatel37
Ěý
It is all about topic of obg for new semester students 
Stability of Dosage Forms as per ICH Guidelines
Stability of Dosage Forms as per ICH GuidelinesKHUSHAL CHAVAN
Ěý
This presentation covers the stability testing of pharmaceutical dosage forms according to ICH guidelines (Q1A-Q1F). It explains the definition of stability, various testing protocols, storage conditions, and evaluation criteria required for regulatory submissions. Key topics include stress testing, container closure systems, stability commitment, and photostability testing. The guidelines ensure that pharmaceutical products maintain their identity, purity, strength, and efficacy throughout their shelf life. This resource is valuable for pharmaceutical professionals, researchers, and regulatory experts.
DIAGNOSIS OF PREGNANCY PPT IN ALL TRIMESTER
DIAGNOSIS OF PREGNANCY PPT IN ALL TRIMESTERdaminipatel37
Ěý
Diagnosis of all three trimester of pregnancy Biography of Dr. Vincenzo Giordano
Biography of Dr. Vincenzo GiordanoDr. Vincenzo Giordano
Ěý
Dr. Vincenzo Giordano began his medical career 2011 at Aberdeen Royal Infirmary in the Department of Cardiothoracic Surgery. Here, he performed complex adult cardiothoracic surgical procedures, significantly enhancing his proficiency in patient critical care, as evidenced by his FCCS certification.
Local Anesthetic Use in the Vulnerable Patients
Local Anesthetic Use in the Vulnerable PatientsReza Aminnejad
Ěý
Local anesthetics are a cornerstone of pain management, but their use requires special consideration in vulnerable groups such as pediatric, elderly, diabetic, or obese patients. In this presentation, we’ll explore how factors like age and physiology influence local anesthetics' selection, dosing, and safety. By understanding these differences, we can optimize patient care and minimize risks.
SAPIENT Medi-trivia Quiz (FINALS) | TRI-ORTA 2025
SAPIENT Medi-trivia Quiz (FINALS) | TRI-ORTA 2025Dr. Anindya
Ěý
Final Round of SAPIENT Medi-trivia quiz
Part of TRI-ORTA 2025
Venue: GLT, Medical College Kolkata
Date: 25-02-2025MORPHOLOGICAL FEATURES OF PNEUMONIA.....
MORPHOLOGICAL FEATURES OF PNEUMONIA.....maheenmazhar021
Ěý
This presentation provides a detailed exploration of the morphological and microscopic features of pneumonia, covering its histopathology, classification, and clinical significance. Designed for medical students, pathologists, and healthcare professionals, this lecture differentiates bacterial vs. viral pneumonia, explains lobar, bronchopneumonia, and interstitial pneumonia, and discusses diagnostic imaging patterns.
đź’ˇ Key Topics Covered:
âś… Normal lung histology vs. pneumonia-affected lung
âś… Morphological changes in lobar, bronchopneumonia, and interstitial pneumonia
âś… Microscopic features: Fibroblastic plugs, alveolar septal thickening, inflammatory cell infiltration
âś… Stages of lobar pneumonia: Congestion, Red hepatization, Gray hepatization, Resolution
âś… Common causative pathogens (Streptococcus pneumoniae, Klebsiella pneumoniae, Mycoplasma, etc.)
âś… Clinical case study with diagnostic approach and differentials
🔬 Who Should Watch?
This is an essential resource for medical students, pathology trainees, and respiratory health professionals looking to enhance their understanding of pneumonia’s morphological aspects.
Creatine’s Untold Story and How 30-Year-Old Lessons Can Shape the Future
Creatine’s Untold Story and How 30-Year-Old Lessons Can Shape the FutureSteve Jennings
Ěý
Creatine burst into the public consciousness in 1992 when an investigative reporter inside the Olympic Village in Barcelona caught wind of British athletes using a product called Ergomax C150. This led to an explosion of interest in – and questions about – the ingredient after high-profile British athletes won multiple gold medals.
I developed Ergomax C150, working closely with the late and great Dr. Roger Harris (1944 — 2024), and Prof. Erik Hultman (1925 — 2011), the pioneering scientists behind the landmark studies of creatine and athletic performance in the early 1990s.
Thirty years on, these are the slides I used at the Sports & Active Nutrition Summit 2025 to share the story, the lessons from that time, and how and why creatine will play a pivotal role in tomorrow’s high-growth active nutrition and healthspan categories.Best Sampling Practices Webinar – USP <797> Compliance & Environmental Monito...
Best Sampling Practices Webinar – USP <797> Compliance & Environmental Monito...NuAire
Ěý
Best Sampling Practices Webinar – USP <797> Compliance & Environmental Monitoring
Are your cleanroom sampling practices USP <797> compliant? This webinar, hosted by Pharmacy Purchasing & Products (PP&P Magazine) and sponsored by NuAire, features microbiology expert Abby Roth discussing best practices for surface & air sampling, data analysis, and compliance.
đź’ˇ Key Topics Covered:
✔️ Viable air & surface sampling best practices
✔️ USP <797> requirements & compliance strategies
✔️ How to analyze & trend viable sample data
✔️ Improving environmental monitoring in cleanrooms
🎥 Watch Now: https://www.nuaire.com/resources/best-sampling-practices-cleanroom-usp-797
📢 Stay informed—follow Abby Roth on LinkedIn for more cleanroom insights!FAO's Support Rabies Control in Bali_Jul22.pptx
FAO's Support Rabies Control in Bali_Jul22.pptxWahid Husein
Ěý
What is FAO doing to support rabies control programmes in Bali, Indonesia, using One Health approach with mass dog vaccination and integrated bite case management as main strategiesDistal End Radius Fractures - Colles, Smiths & Bartons
- 2. • Colles’ Fracture • Smith’s Fracture • Barton’s Fracture
- 3. • Described by Abraham Colles in 1814. • It is the most common of all fractures in elderly. • Usually in older women. • Fall on a out stretched hand.
- 4. Colles’ Fracture It is a Transverse fracture of the distal end of the radius at its Cortico-Cancellous Junction with typical Dorsal Displacement of the distal fragment.
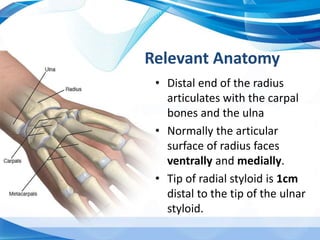
- 5. • Distal end of the radius articulates with the carpal bones and the ulna • Normally the articular surface of radius faces ventrally and medially. • Tip of radial styloid is 1cm distal to the tip of the ulnar styloid. Relevant Anatomy
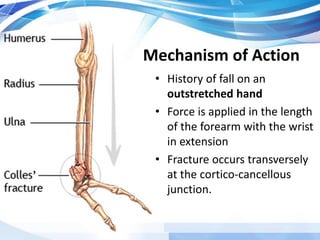
- 6. Mechanism of Action • History of fall on an outstretched hand • Force is applied in the length of the forearm with the wrist in extension • Fracture occurs transversely at the cortico-cancellous junction.
- 7. The distal fragment collapses into- • Dorsal Displacement • Dorsal Tilt • Lateral/Radial Displacement • Lateral/ Radial Tilt • Supination • Impaction of Fragments Also associated with extension and shortening.
- 8. Associated injuries • Fracture of styloid process of ulna • Rupture of the Ulnar collateral ligament • Rupture of the triangular Fibro-cartilage complex (TFCC) of ulna. • Rupture of the interosseos, radio-ulnar ligament causing radio-ulnar subluxation.
- 9. Clinical Features • Pain, tenderness, swelling and irregularity of the lower end of radius. • “Dinner Fork Deformity” • Radial styloid comes at the level of the ulnar styloid.
- 11. Radiological findings • Transverse fracture of the distal end radius at cortico- cancellous junction. • The distal fragment shows – a)Dorsal tilt & displacement – Lateral View b)Lateral tilt & Displacement – AP View • Maybe associated with communition or broken ulnar styloid process.
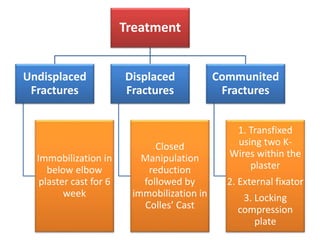
- 14. Treatment Undisplaced Fractures Immobilization in below elbow plaster cast for 6 week Displaced Fractures Closed Manipulation reduction followed by immobilization in Colles’ Cast Communited Fractures 1. Transfixed using two K- Wires within the plaster 2. External fixator 3. Locking compression plate
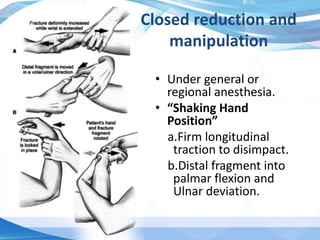
- 15. Closed reduction and manipulation • Under general or regional anesthesia. • “Shaking Hand Position” a.Firm longitudinal traction to disimpact. b.Distal fragment into palmar flexion and Ulnar deviation.
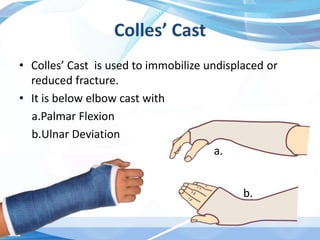
- 16. Colles’ Cast • Colles’ Cast is used to immobilize undisplaced or reduced fracture. • It is below elbow cast with a.Palmar Flexion b.Ulnar Deviation a. b.
- 20. Complications Early • Circulatory Problems • Carpal tunnel syndrome – Median Nerve injury • Reflex sympathetic dystrophy • TFCC injury • Subluxation of inferior radio ulnar joint Late • Malunion • Delayed Union and Non-union • Stiffness • Extensor Pollicis Longus Tendon rupture
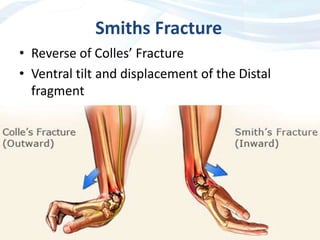
- 21. Smiths Fracture • Reverse of Colles’ Fracture • Ventral tilt and displacement of the Distal fragment
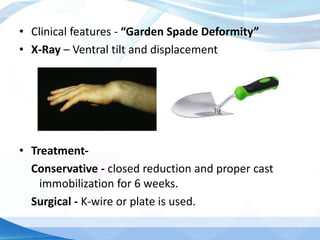
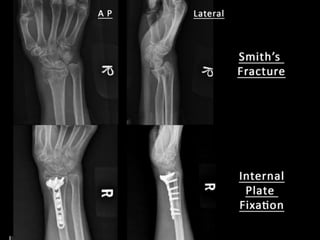
- 22. • Clinical features - “Garden Spade Deformity” • X-Ray – Ventral tilt and displacement • Treatment- Conservative - closed reduction and proper cast immobilization for 6 weeks. Surgical - K-wire or plate is used.
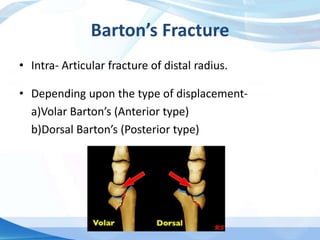
- 24. Barton’s Fracture • Intra- Articular fracture of distal radius. • Depending upon the type of displacement- a)Volar Barton’s (Anterior type) b)Dorsal Barton’s (Posterior type)
- 25. • Extends from articular surface of the radius to either its anterior and posterior cortices. • The small distal fragment is displaced along with the carpals. • Treatment a) Closed Reduction and Plaster Cast b) Internal Fixation by Plate or K-wire
- 26. Apley’s System of Orthopaedics and Fractures – 9th edition Essential Orthopaedics – Maheshwari & Mhaskar – 5th edition